Download as PDF, PPTX

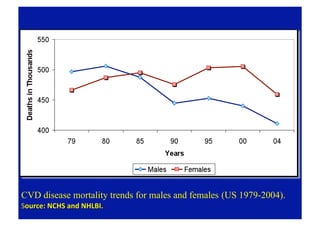
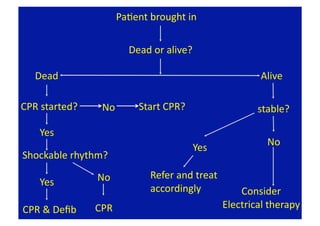
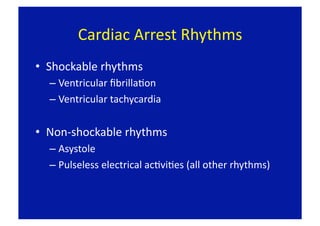
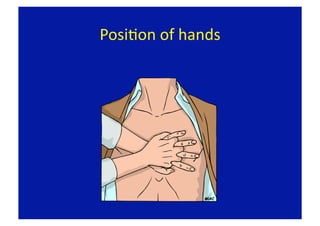
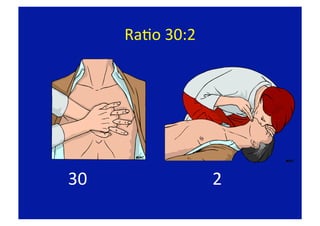
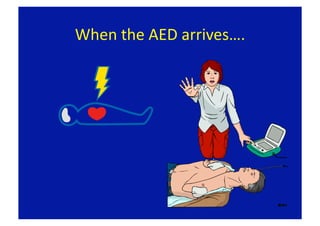
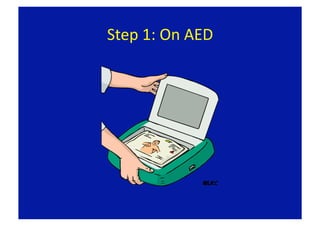
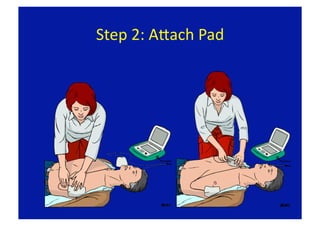
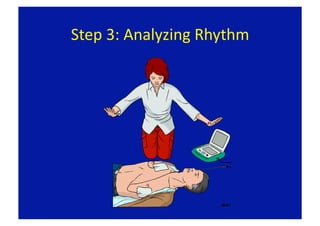
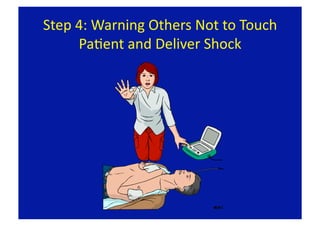
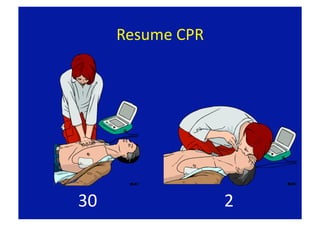
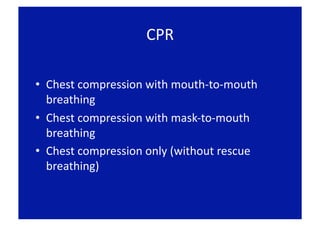


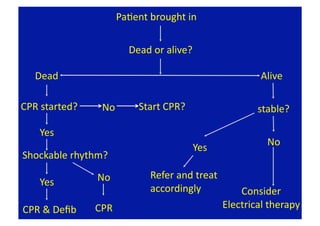
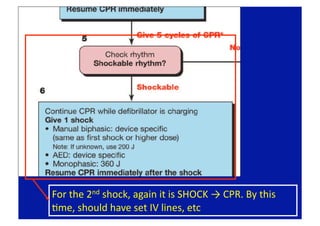
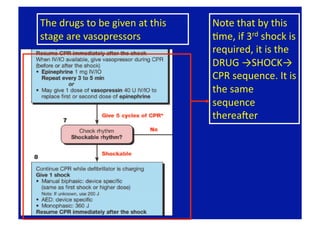
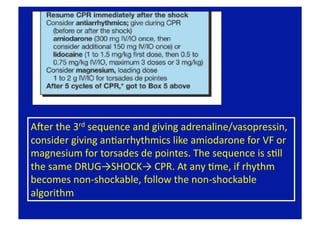










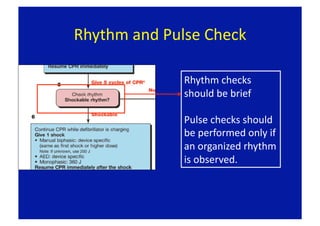

This document provides an overview of basic and advanced life support techniques according to 2005 American Heart Association guidelines. It discusses the importance of early defibrillation and effective bystander CPR for cardiac arrest survival. The chain of survival emphasizes early recognition, early CPR, early defibrillation, and early advanced life support. Hands-only CPR is presented as an option for untrained rescuers performing bystander CPR. Advanced life support techniques are outlined, including treatment approaches for shockable and non-shockable rhythms.











































































































