Downloaded 27 times











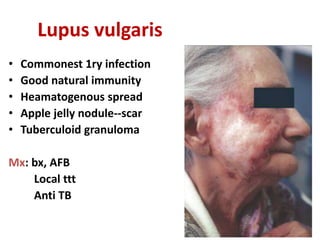
![• primary TB infection
[tuberculous chancre]
• Lupus vulgaris
Scrofuloderm](https://image.slidesharecdn.com/bacterialinfectionsoftheskin-170509113450/85/Bacterial-skin-infections-55-320.jpg)
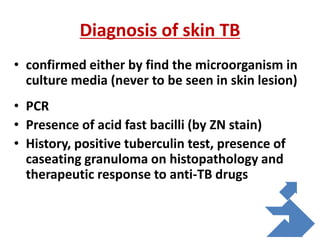
![• Tuberculous warts:
[tuberculosis
verrucosa cutis]
• Orificial TB
• Papulonecrotic
tuberculide
Lichen scrofulosorum
Erythema induratum](https://image.slidesharecdn.com/bacterialinfectionsoftheskin-170509113450/85/Bacterial-skin-infections-56-320.jpg)


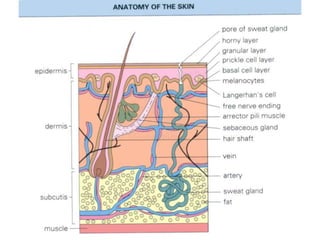
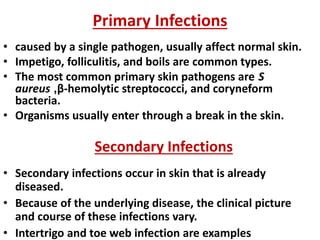
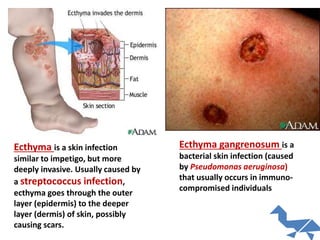
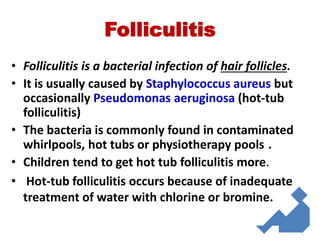
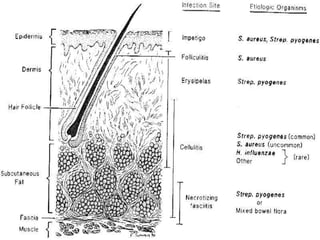
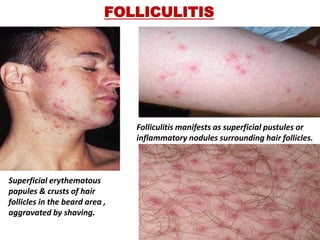
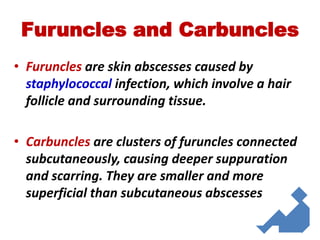
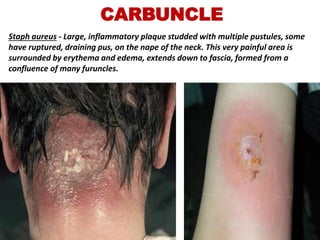
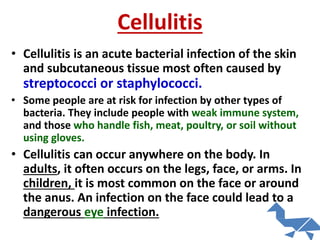
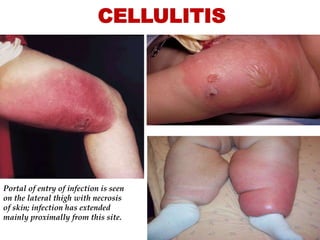
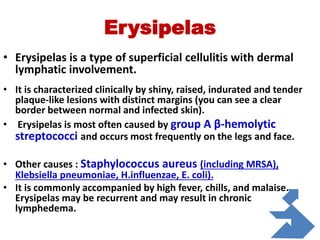
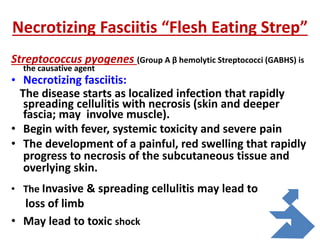
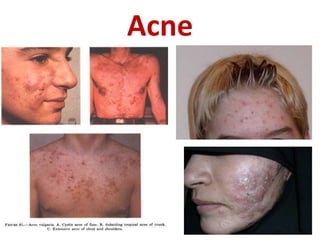
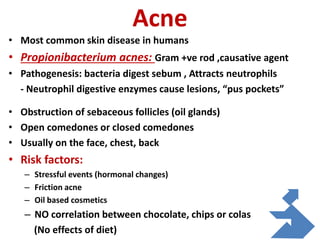
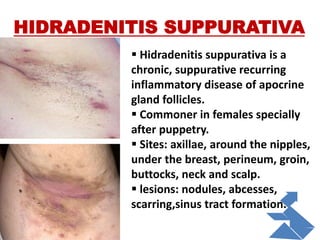
Bacterial infections of the skin can be primary, caused by a single pathogen affecting normal skin, or secondary, occurring in already diseased skin. Common primary bacterial skin infections include impetigo, folliculitis, and boils, often caused by Staphylococcus aureus or streptococci. Secondary infections may involve the skin folds, and include conditions like intertrigo and toe web infections. Specific bacterial infections are impetigo, folliculitis, furuncles, carbuncles, cellulitis, erysipelas, cutaneous abscesses, and necrotizing fasciitis. Acne is also discussed as an infection of hair follicles by Propionibacterium acnes.

















![1.1.1. bacterial infection of skin [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/1-1-1-bacterialinfectionofskincompatibilitymode-130325014737-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)





































































