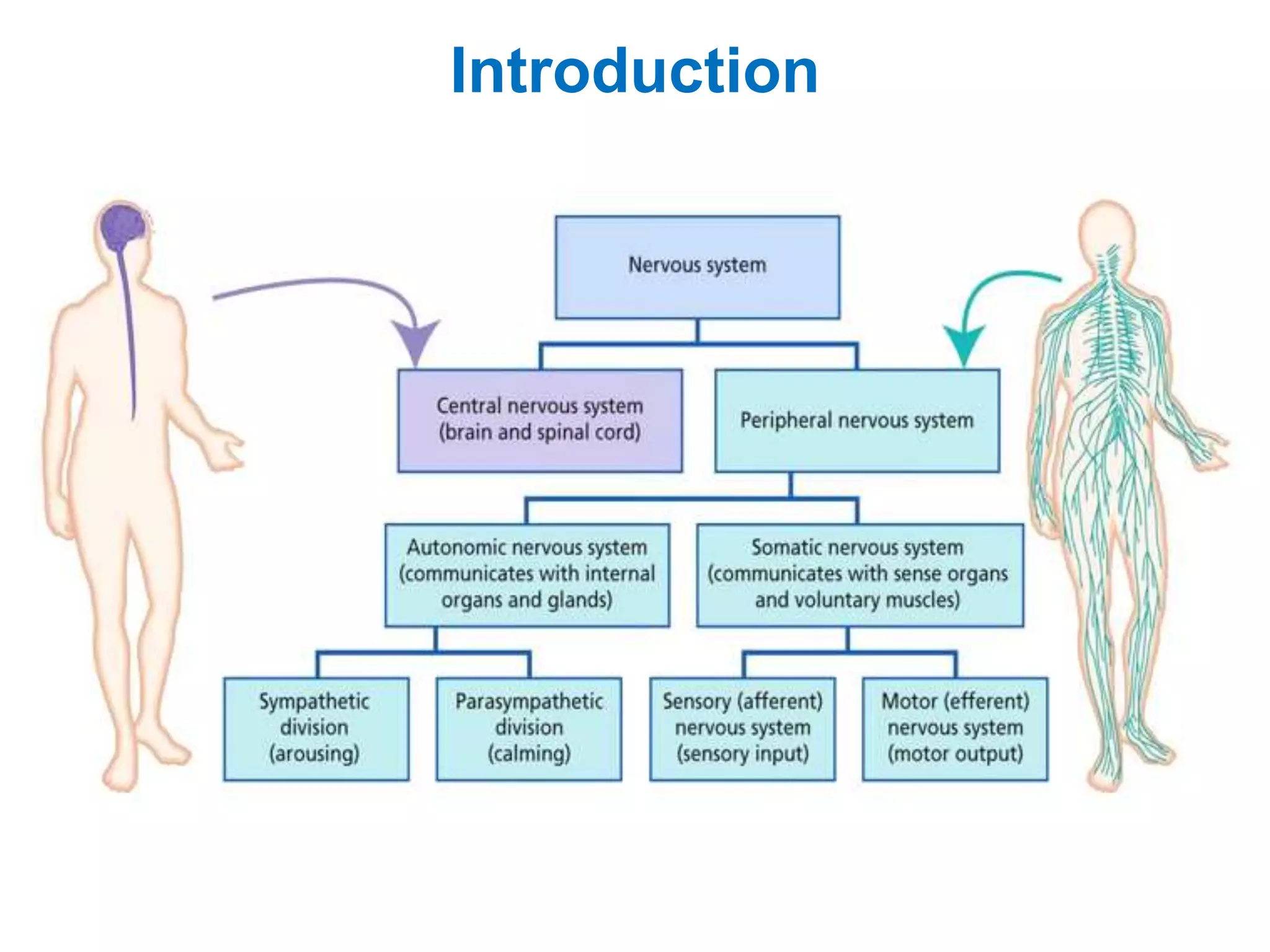
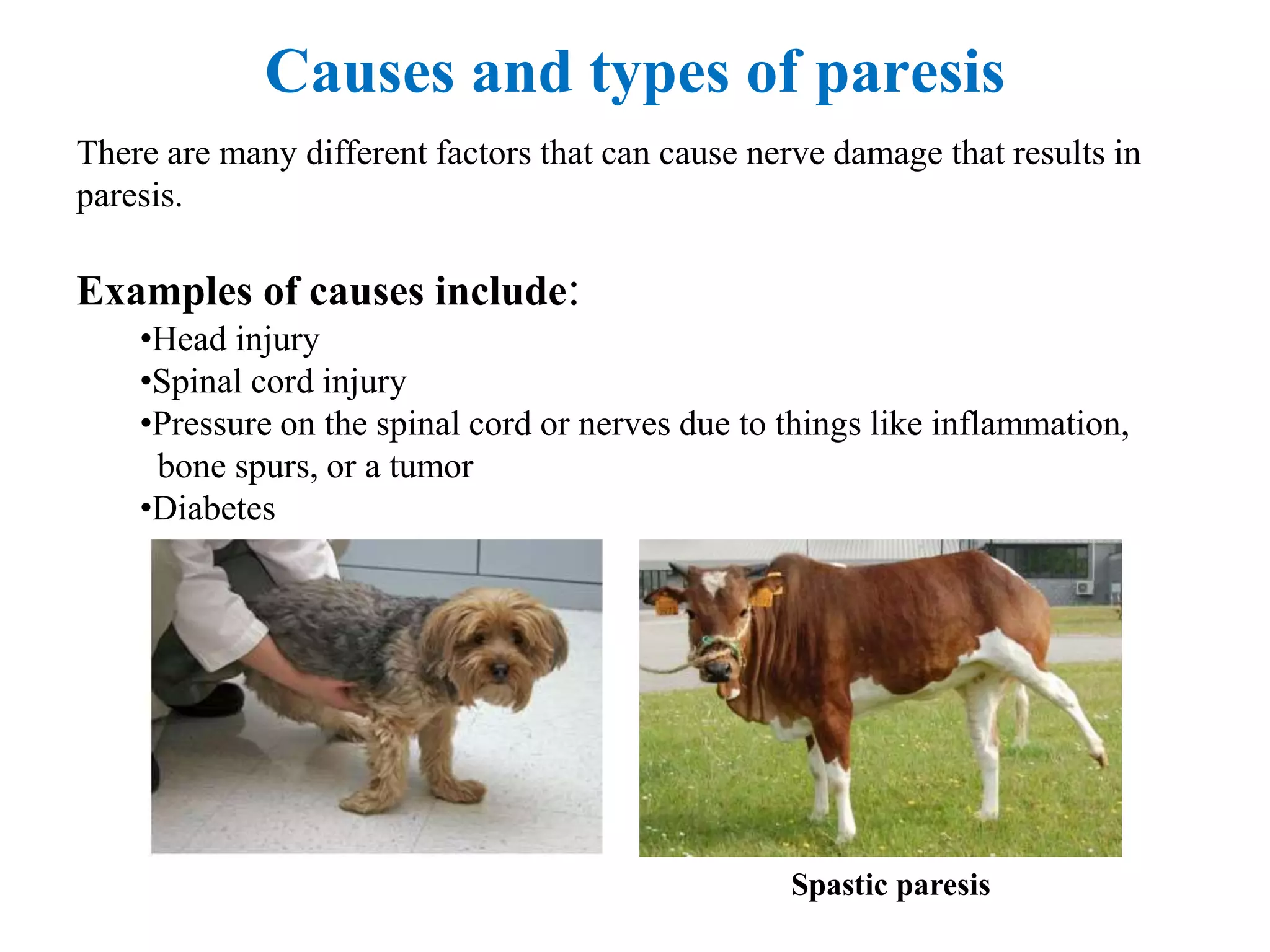
The document discusses diseases of the nervous system in animals. It describes how veterinary neurologists treat problems of the brain, spinal cord, nerves and muscles. Neurological issues in animals can be caused by medication reactions, inherited disorders, infections or trauma. Common conditions include seizures, brain/spinal tumors, meningitis, congenital disorders, and disk problems. A neurological exam involves taking a patient history and doing palpation, percussion and image analysis. Treatment depends on the underlying cause but may include surgery, medications, antibiotics or chemotherapy. The document also discusses various neurological signs like changes in behavior, physical changes, involuntary movements and abnormal posture/gait.