Downloaded 37 times




![Clinical Investigations: MD Rules 2017
• Although the medical devices rules 2017 does not give any details of data
requirements for clinical investigations medical devices, they do mention
and give at least three clear indications:
• 1. A pilot clinical investigation meaning a clinical study may have to be carried out
for the first time in human beings
• A pivotal clinical investigation meaning a confirmatory clinical trial based on the
data emerging from pilot clinical trial [may have to be carried out for Class C & D]
• 3. Medical devices requiring clinical trials but claiming substantial equivalence
cannot be marketed without official approval](https://image.slidesharecdn.com/profbcctrequirementsmeddevices27dec2018-190101090949/75/Clinical-Trial-Requirements-Medical-Devices-27-dec2018-7-2048.jpg)















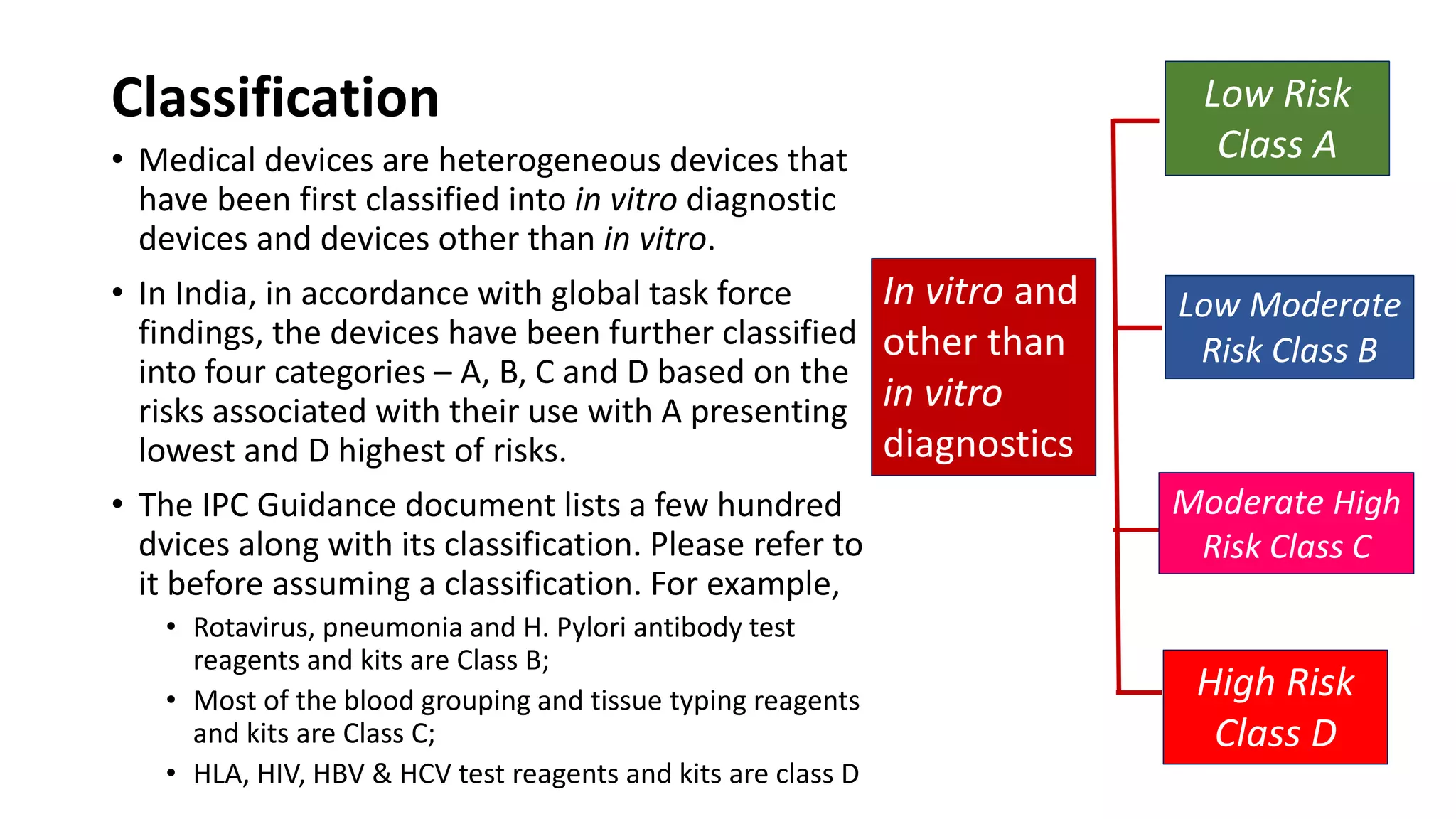
The document outlines the clinical trial requirements for market approval of medical devices in India, highlighting the classification of devices into risk categories and the need for clinical investigations under the Medical Devices Rules 2017. It discusses the absence of detailed data requirements in official guidance while emphasizing the significance of pilot and pivotal clinical trials for various classes of devices. A case study on the Micra transcatheter pacing system illustrates the clinical endpoints for efficacy and safety, demonstrating the need for rigorous evaluation and statistical analysis in trial design.









































![Educo Life Science [gathering clinical evidence] [module 1]](https://cdn.slidesharecdn.com/ss_thumbnails/educo-gatheringclinicalevidence-module1-220128131137-thumbnail.jpg?width=640&height=640&fit=bounds)













































