
Recommended
More Related Content
What's hot
What's hot (20)
Similar to ACCOMMODATION 2.pptx
Similar to ACCOMMODATION 2.pptx (20)
More from bakanangemmahpholoan
More from bakanangemmahpholoan (20)
Recently uploaded
Recently uploaded (20)
ACCOMMODATION 2.pptx
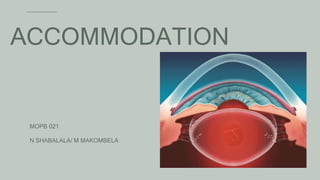
- 1. ACCOMMODATION MOPB 021 N SHABALALA/ M MAKOMBELA
- 2. CONTENT 01 Introduction & Background 02 Mechanism of Accommodation 03 Accommodation Pathway 04 Types of accommodation 05 Amplitude of Accommodation 06 Accommodation Response 07 Accommodative Facility 08 Anomalies of Accommodation 4/12/2023 2
- 3. 01 INTRODUCTION & BACKGROUND 4/12/2023 3 Accommodation: Is the mechanism by which the eye changes refractive power by altering the shape of lens in order to focus objects at variable distances Far point: Position of an object when its image clearly falls on retina with no accommodation. Near point: Nearest point clearly seen with maximum accommodation. Range of accommodation: Distance between far point and near point.
- 4. 4/12/2023 4 THEORIES OF ACCOMMODATION 01 Relaxation theory of HELMHOLTZ 02 SCHACHAR’S theory 03 TSHERNING’S theory 04 CATENARY theory
- 5. Relaxation theory of HELMHOLTZ • Also known as the “Capsular Theory”. • He considered that lens was elastic and in normal state it is stretched and flattened by tension of the suspensory ligaments. • During accommodation, contraction of ciliary muscle shortens ciliary ring and moves towards the equator of the lens. • Relax the suspensory ligaments, relieving strain. • Lens assumes more spherical form, increasing thickness and decreasing diameter. 4/12/2023 5
- 6. Relaxation theory of HELMHOLTZ • Imaging technique showed that ciliary muscle move anteriorly & the equatorial edge of lens move away from sclera during accommodation. • Zonular fibers extending from ciliary processes to lens equator, are relaxed during accommodation • It is not clear how lens alters its shape when tension in suspensory ligaments is relaxed 4/12/2023 6
- 7. SCHACHAR’S theory • Presbyopia is due to growth in equatorial diameter, leads to decrease in perilenticular space • Contraction of ciliary muscle cannot tense zonules and expand lens coronally. • SCHACHAR introduced use of scleral expansion bands (SEB) 4/12/2023 7
- 8. TSHERNING’S theory • This theory attributed increased curvature of capsule to increasing tension of the zonules. • It states that contraction of ciliary muscle pulls zonules directly and increases tension of capsule at equator of lens, which leads to bulging of poles. 4/12/2023 8
- 9. COTENARY theory • Proposed by COLEMAN • The COTENARY (hydraulic suspension) theory proposes that lens, zonules & anterior vitreous comprise a diaphragm between aqueous and vitreous • As ciliary muscle contracts it forms a pressure gradient, causing anterior movement of lens zonules diaphragm and increasing anterior central curvature. • Presbyopia is due to increase in lens volume, results in reduced response to pressure gradient created by ciliary body contraction. 4/12/2023 9
- 10. 02 MECHANISM OF ACCOMMODATION 4/12/2023 10 When the eyes are fixed on a distant object: • Lens is flat due to the traction of suspensory ligaments When vision is shifted from the distant object to a near object: • Ciliary muscle contracts • Stimulation of the parasympathetic nerves contracts both sets of ciliary muscle fibers • The contraction of the ciliary muscle relaxes the suspensory ligaments, and the lens assumes a more spherical shape
- 11. 03 ACCOMMODATION PATHWAY 4/12/2023 11 The association fibers carry the impulses to frontal lobe. The center for accommodation lies in: frontal eye field (area 8) that is situated in the frontal lobe of cerebral cortex Receptors: RODS & CONES -> Visual impulses from retina pass through the optic nerve ->optic chiasma -> optic tract-> lateral geniculate body -> optic radiation to visual cortex (area 17) of occipital lobe -> frontal eye field (area 8) AFFERENT PATHWAY
- 12. ACCOMMODATION PATHWAY 4/12/2023 12 Efferent fibers to medial rectus: Some of the fibers from frontal eye field terminate in the somatic motor nucleus of oculomotor nerve. The fibers from motor nucleus supply medial rectus. Efferent fibers to ciliary muscle and sphincter pupillae: From area 8, the corticonuclear fibers pass via internal capsule to the Edinger-Westphal nucleus of third cranial nerve. The preganglionic fibers pass through the third cranial nerve to ciliary ganglion. Postganglionic fibers from ciliary ganglion pass via the short ciliary nerves and supply the ciliary muscle and the constrictor pupillae. EFFERENT PATHWAY From Area 8-> EWN of CN3-> Ciliary Ganglion -> Short Ciliary Nerve -> Ciliary muscle-> Increase in anterior curvature of lens
- 14. 04 TYPES OF ACCOMMODATION 4/12/2023 14 01 Tonic Accommodation 02 Proximal Accommodation 03 Reflex Accommodation 04 Convergence-accommodation
- 15. 4/12/2023 15 TYPES OF ACCOMMODATION Tonic accommodation It is due to tonus of ciliary muscle and is active in absence of a stimulus The resting state of accommodation is not at infinity but rather at an intermediate distance
- 16. 4/12/2023 16 TYPES OF ACCOMMODATION Proximal accommodation Is induced by the awareness of the nearness of a target. This is independent of the actual dioptric stimulus
- 17. 4/12/2023 17 TYPES OF ACCOMMODATION Reflex accommodation Is an automatic adjustment response to blur. It is made to maintain a clear and sharp retinal image
- 18. 4/12/2023 18 TYPES OF ACCOMMODATION Convergence-accommodation Amount of accommodation stimulated or relaxed associated with convergence The link between accommodation and convergence is known as accommodative convergence and is expressed clinically as AC/A ratio.
- 19. 05 AMPLITUDE OF ACCOMMODATION 4/12/2023 19 01 Push up to blur test 02 Minus lens to blur 03 Pull away to clear test 04 Monocular Estimate Method DEFINITION Amplitude of accommodation (AoA) is the maximum increase in optical power that an eye can achieve in adjusting its focus from far to near
- 20. 4/12/2023 20 Purpose To determine maximum amount of accommodation that eyes are capable of producing individually or together Procedure: Near visual acuity chart placed on near point rod/RAF Ruler Direct patient’s attention to 20/20 line of letters on near point card . Patient left eye occluded Near point card brought closer to patient (2-3 inches per second) Patient instructed to keep the letters as clear as possible and report when it blurs. Prompt the patient to clear the target Stop when patient can no longer clear the print within 2 to 3 seconds of viewing. Record the dioptric points on the near point rod that corresponds with the blur. Procedure repeated for left eye Amp (D) = 100/distance (cm) PUSH-UP TO BLUR TEST
- 21. 4/12/2023 21 SETUP Patient is seated comfortably behind the phoropter viewing through his or her distance prescription. A well-illuminated near target (one line of letters larger than the patient’s near visual acuity) is set at 40 cm. Testing is done monocularly only. PROCEDURE Instructions to patient: “I will be changing the lenses in front of your eyes. Try to clear the print after each lens change. Tell me when you notice that the letters [examiner indicates appropriate print] are slightly blurred, still readable, but cannot be cleared by further effort.” Minus lenses are added in 0.25 D increments. When the patient reports first sustained blur, the lens power is noted. To obtain the amplitude in diopters, add 2.50 D for working distance to the amount of minus added. • e. g Minus added until first sustained blur −6.00 D. Working distance (40 cm) −2.50 D. Accommodative amplitude −8.50 D MINUS LENS METHOD
- 22. 4/12/2023 22 SETUP Ambient and overhead lighting should provide good illumination. The line above best VA on a near card is used as the target. The examiner should hold the target very close to the eye to begin the test. If the patient wears glasses, these should be used. Occlude the patient’s left eye. PROCEDURE To begin the test, slowly move the target away from the patient’s eye at approximately 1 to 2 cm/sec. The target will be moved away from the patient until they can just report the letters. This will be considered the endpoint. Measure the distance from the eye to the stick. The accommodative amplitude will be measured to the nearest centimeter. Amp (D) = 100/distance (cm) PULL AWAY TO CLEAR TEST
- 23. 4/12/2023 23 1. The distance prescription in on. 2. The patient is asked to fixate on an appropriate target on the MEM card attached to the retinoscope head. 3. The examiner then moves closer to the patient observing the reflex. 4. If the initial reflex at the patient's Harmon's distance was a with movement, then the amplitude is reached when a change to a more "with" movement is observed. This distance is then converted to a dioptric value from the spectacle plane which is indicated of the patient's amplitude. 5. If the initial reflex was against, the amplitude is reached when there is a change to a with movement, the distance of which is then converted to a dioptric value. Amp (D) = 100/distance (cm) MONOCULAR ESTIMATE METHOD
- 24. 4/12/2023 24 • Hofstetter formulae for expected amplitude as a function of age (using the data of Donders, Duane and Kaufman) • Maximum amplitude = 25 - 0.4(age) • Probable (average pt should have) amplitude = 18.5 – 1/3 (age) • Minimum amplitude = 15 - 0.25(age) NORMAL VALUES
- 25. 4/12/2023 25 • Example : • For 20 years old patient Minimum AA is given by : 15 – 0.25 *age • = 15 – 0.25 *20 • = 10 D HOFSTETTER FORMULAE
- 26. 4/12/2023 26 • The change in accommodative convergence that occurs when the patient accommodates or relaxes accommodation by a given amount. • Determination of the AC/A ratio is important in analysis of optometric data. • The AC/A finding is a key characteristic in the final determination of the diagnosis. • It is also one of the most important findings used to determine the appropriate management sequencefor any given condition. • Norms 4 to 6 : 1 AC/A RATIO
- 27. 4/12/2023 27 • There are two methods for determining a patient’s AC/A ratio. • The first, referred to as the calculated AC/A ratio, is determined using the following formula: • AC/A = IPD (cm) + NFD (m) (Hn − Hf ) where • IPD = interpupillary distance in centimeters • NFD = near fixation distance in meters • Hn = near phoria (eso is plus and exo is minus) • Hf = far phoria (eso is plus and exo is minus) • Example: IPD = 60 mm, the patient is 2 exophoric at distance and 10 exophoric at near (40 cm). • AC/A = 6 + 0.4(−10 + 2) • = 6 + 0.4(−8) = 6 + (−3.2) • = 2.8 When using this formula, one should remember to use the correct signs for esophoria and exophoria. AC/A RATIO
- 28. 4/12/2023 28 • The second method, called the gradient AC/A, is determined by measuring the phoria a second time using −1.00 or −2.00 lenses. • The change in the phoria, with the additional minus, is the AC/A ratio. • (Phoria 1 – phoria 2) / lens • For example, if the near phoria is 2 esophoria through the subjective finding and, with −1.00, it is 7 esophoria, the AC/A ratio is 5:1. (2-7)/-1 =-5/-1 =5 Therefore AC/A ratio 5:1 AC/A RATIO
- 29. 4/12/2023 29 • The effect of proximal convergence and the lag of accommodation result in calculated AC/A ratio and gradient AC/A ratio being different. • The calculated AC/A ratio is usually larger than the gradient because of the effect of proximal vergence, which affects the near phoria measurement. • Because the gradient ratio is measured by testing the near phoria twice at a fixed distance, proximal vergence is held constant and theoretically does not alter the final result. • The lag of accommodation also accounts for differences between the calculated and gradient AC/A ratio measurements. Although the stimulus to accommodation is 2.50 D at near, the accommodative response is typically less than the stimulus. • This difference between the stimulus and response of the accommodative system is called the lag of accommodation. The lag of accommodation is generally +0.25 to +0.75 D. Because the patient will tend to underaccommodate for any given stimulus, the gradient AC/A tends to be lower than the calculated AC/A ratio. AC/A RATIO
- 30. 4/12/2023 30 • The extent to which a patient is able to stimulate (PRA) or relax (NRA) their accommodation • The primary objective of these tests is to determine whether the patient requires an add for near work. • The test is also used with the presbyopic population to determine if an add is necessary and to finalize the magnitude of the required add. • The NRA can also be used to determine whether a patient has been overminused during the subjective examination. • The NRA is performed through the subjective prescription, which should eliminate all accommodation at distance. • Because the test distance is 40 cm, the patient will accommodate approximately 2.5 D to see the target clearly. Therefore, the maximum amount of accommodation that can be relaxed is 2.50 D. • Thus, an NRA finding greater than +2.50 suggests that the patient was overminused. • It is important to ask the patient to keep the target clear and single during these tests. Traditionally, the instructional set is, “As I add lenses in front of your eyes, keep these letters clear for as long as you can. Tell me when the letters are blurry.” • It is important to also ask the patient to report diplopia, because these tests also indirectly probe the ability to maintain fusion using positive and negative fusional vergence. • The endpoint for the PRA will vary depending on the patient’s amplitude of accommodation, AC/A ratio, and the negative fusional vergence. • The expected values for NRA are +2.00, ±0.50; for PRA, the expected values are −2.37, ±1.00. NRA/PRA
- 31. 06 ACCOMMODATION RESPONSE 4/12/2023 31 DEFINITION Measure of actual accommodation that is present Accommodative stimulus - Measure of accommodation exerted by target or stimuli Lag of accommodation = Accommodative stimulus – Accommodative response
- 32. 4/12/2023 32 • When evaluating the accommodative or binocular systems, we usually present the stimulus at 40 cm. This creates an accommodative demand of 2.50 D. This is referred to as the stimulus to accommodation.’ • Although the stimulus to accommodation is 2.50 D, the accommodative response will generally be about 10% less than the stimulus (25). • The expected finding for MEM retinoscopy, for example, which assesses the accommodative response, is a lag of accommodation of about +0.25 to +0.50 D. • It is important to be aware of the difference between the response and stimulus to accommodation, realizing that most patients will underaccommodate by about 10%. An instance where this becomes important is when comparing the calculated AC/A ratio to the gradient AC/A ratio. ACCOMMODATION RESPONSE
- 33. 4/12/2023 33 • The working distance should be at 40 cm for adults or at the Harmon distance (the distance from the patient’s elbow to the middle knuckle) for children. • Select an MEM card that is appropriate for the age and grade level of the patient. • While the patient reads the words on the card, perform retinoscopy along the horizontal axis and estimate the amount of plus or minus necessary to neutralize the motion of the retinoscopic reflex observed. • A lens can be quickly placed before the eye being evaluated to confirm the estimate. • It is important, however, not to leave the lens in place too long because it can alter the accommodative response. • Interpretation of the results of MEM testing is based on the assumption that the accommodative stimulus at distance has been reduced to zero. If the patient is not wearing the subjective or has been overcorrected or undercorrected, interpretation of the MEM result will be affected. MONOCULAR ESTIMATED METHOD
- 34. 4/12/2023 34 • When performing MEM retinoscopy, it is important to use normal room illumination. • Accommodation is affected by illumination (e.g., dark focus), and dim illumination will alter the accommodative response. Accommodation should therefore be tested under illumination that the patient habitually uses. • The expected value for MEM retinoscopy is +0.25 D to +0.50 D MONOCULAR ESTIMATED METHOD
- 35. 4/12/2023 35 • Any testing performed under binocular conditions is affected by both accommodative and binocular function. • Thus, although MEM is considered a test of accommodative function, binocular vision is also being assessed. For example, a finding of less plus than expected may reflect overaccommodation secondary to accommodative excess or high exophoria and decreased positive fusional vergence. • A patient with high exophoria and inadequate positive fusional vergence may use accommodative convergence to supplement the inadequate fusional vergence. This would enable the individual to maintain binocularity, although it may lead to blurred vision secondary to the overaccommodation. • The same reasoning applies to a finding of more plus than expected on MEM retinoscopy. This could suggest either underaccommodation secondary to accommodative insufficiency or high esophoria and reduced negative fusional vergence. ACCOMMODATION RESPONSE
- 36. 4/12/2023 36 • PURPOSE: To evaluate the accommodative response of a patient while viewing a near target under binocular conditions. • Because the fused cross-cylinder test is a subjective method, it is difficult to use with children younger than 8 to 9 years. It is generally easier and faster to perform MEM retinoscopy. This test is also not as repeatable as MEM retinoscopy • The expected value for the binocular fused cross-cylinder test is +0.50 D with a standard deviation of ±0.50 D • High lag >+0.75D Lead of Accommodation < +0.25D • This test finds the amount of plus that makes the accommodative stimulus and accommodative response equal • Generally higher plus is found in high lag of accommodation and minus is found in lead of accommodation cases • Presbyopes: this test provides the examiner with a tentative bifocal add FUSED CROSS-CYLINDER TEST
- 37. 4/12/2023 37 • SET-UP: • Phoropter at near PD setting • crossed cylinder grid placed @ 40 cm • Turn auxiliary to +0.50 crossed cylinder • Room light off, stand light illumination on • Ask patient “Are ‘up and down’ or ‘across’ lines clearer, blacker, or sharper ?” • If ‘across’ (horizontal) lines clearer - Under accommodation - So, add plus power binocularly until patient reports equality or vertical lines become clearer • If ‘up and down’ (vertical) lines clearer - Over accommodation - So, add minus power binocularly until patient reports equality FUSED CROSS-CYLINDER TEST
- 38. 07 ACCOMMODATIVE FACILITY 4/12/2023 38 DEFINITION Aka inertia of accommodation Tests the ease of accommodative response to the change in stimulus. To determine flexibility of accommodative system Testing accommodative facility provides an index of how quickly accommodation can change
- 39. 4/12/2023 39 Measured in cycles per minute Flipper Lens Test Flipper lens - Two plus and two minus lenses mounted in same holder - Available in powers of : +/- 0.50, 1.00, 1.50, 2.00, 2.50, 3.00 Purpose To determine the ability of accommodative system to respond to lens created blur with a monocular stimulus presentation Note : In the binocular presentation, the ability of both accommodative and vergence systems to interact is tested Flipper Lens Test ACCOMMODATIVE FACILITY
- 40. 4/12/2023 40 Patient holds near-point VA chart with 20/25 letters at 40 cm Direct light from overhead lamp Distance correction worn Left eye occluded Flipper lens placed in front of right eye(usually minus side first) Procedure As soon as letters on acuity chart becomes clear, it is flipped to other side i.e. plus side As letters become clear with plus side flip back lens to minus Continue the procedure for 30 seconds The process repeated for left eye for 30 seconds ACCOMMODATIVE FACILITY
- 41. 4/12/2023 41 • Record and interpretation • Record no. of cycles in a minute 1 cycle = plus to minus and back to plus again • Expected Monocularly minimum = 12 cycles per min average = 17 cycles per min • Binocularly minimum = 10 cycles per min average = 13 cycles per min • Near-Far test- Read up (SS) ACCOMMODATIVE FACILITY
- 43. 4/12/2023 43 Classification (by Duane) • Insufficiency of accommodation • Ill-Sustained accommodation • ACCOMMODATION INFACILITY • Excessive accommodation • Spasm of accommodation • Presbyopia ANOMALIES OF ACCOMMODATION
- 44. 4/12/2023 44 • Condition in which accommodative power is constantly less than lower limit of normal range according to patient’s age Etiology • Premature sclerosis of lens • Weakness of ciliary muscle due to systemic causes: Debilitating illness, anemia, toxemia, malnutrition, dia betes mellitus, pregnancy, stress etc. • Weakness of ciliary muscle due to local causes: PAOG, mild cyclitis as during onset of sympathetic ophthalmia. INSUFFICIENCY OF ACCOMMODATION
- 45. 4/12/2023 45 • Clinical features • Features of eye strain and asthenopia. • Head ach, fatigue & irritability of the eyes, while attempting near work. • Near work is blurred & becomes difficult or impossible. • Disturbance of convergence : intermittent diplopia. • It is stable condition, if due to sclerosis of lens. • But is not stable in association with ciliary muscle weakness INSUFFICIENCY OF ACCOMMODATION
- 46. 4/12/2023 46 Treatment • Identification & treatment of any systemic cause. • Any refractive error should be corrected & if vision for near work is seriously blurred then additional near correction has to be prescribed same as presbyopia. • If associated with convergence excess then full spherical correction. • Convergence insufficiency is there, then base in prisms can be added. • Prismatic correction added should bring near point of convergence to same distance as near point of accommodation. • Weakest convex lenses should be prescribed, so as to exercise and stimulate accommodation. • After recovery additional correction should be made weaker and weaker from time to time. INSUFFICIENCY OF ACCOMMODATION
- 47. 4/12/2023 47 • Accommodative exercises: • While doing exercises patient should wear correction for distance. • Should be done simultaneously in both eyes, even if associated with convergence insufficiency. • But with convergence excess then the exercise should done with one eye alternately. • Accommodation test card exercise. (HART Charts) • Useless in generalized debility and sclerosis of lens. INSUFFICIENCY OF ACCOMMODATION
- 48. 4/12/2023 48 • Aka accommodation fatigue • It is a situation in which though range of accommodation is in normal range but it cannot sustain it for a sufficient period of time. • Initial stage of insufficiency of accommodation It occurs due to • Stage of convalescence from debilitating illness • Stage of generalized tiredness ILL-SUSTAINED ACCOMMODATION
- 49. 4/12/2023 49 Clinical features • These symptoms are most commonly reported at the end of the day • Blurred vision after prolonged near work. • Headaches • Eyestrain • Fatigue, sleepiness and a loss of comprehension with continued reading • A dull 'pulling' sensation around the eye. ILL-SUSTAINED ACCOMMODATION
- 50. 4/12/2023 50 Treatment • Near work should be curtailed during debilitating illness. • General tonic measures should be taken. • The condition of illumination and posture while doing near work, should be improved. ILL-SUSTAINED ACCOMMODATION
- 51. 4/12/2023 51 • It is a condition in which patient faces difficulty in altering the range of accommodation. • Amplitude of accommodation is normal. • Ability to make use of this amplitude quickly and for long periods of time is inadequate. ACCOMMODATION INFACILITY
- 52. 4/12/2023 52 Clinical features • Difficulty changing focus from one distance to another • Headaches • Eyestrain • Fatigue • Difficulty sustaining near tasks • Blurred vision Treatment: correcting any refractive error and accommodative exercises. ACCOMMODATION INFACILITY
- 53. 4/12/2023 53 • Accommodative response is greater than the accommodative stimulus • There is functional increase in tonus of ciliary muscle, results in a constant accommodative effect Causes • Young hypermetropes frequently uses excessive accommodation as a physiological adaptation • Young myopes performing excessive near work, associated with excessive convergence. • Astigmatic error in young patients • Presbyopes in the beginning • Use of improper and ill fitting spectacles EXCESSIVE ACCOMMODATION
- 54. 4/12/2023 54 Precipitating factors • Excessive near work done, especially in dim or excessive illumination. • General debility, physical or mental ill health Symptoms Blurred vision at near is uncommon Blurred vision at distance Headaches Eyestrain Photophobia Difficulty changing focus from distance to near Diplopia EXCESSIVE ACCOMMODATION
- 55. 4/12/2023 55 • Treatment • It has a good prognosis. • Refractive error should be corrected after carefully performed cycloplegic refraction. • Near work should be stopped for some time, after that it should be done with proper illumination conditions. EXCESSIVE ACCOMMODATION
- 56. 4/12/2023 56 • Spasm of accommodation refers to exertion of abnormally excessive accommodation. Causes • Drug induced spasm of accommodation is known to occur after use of strong miotics. • Spontaneous spasm of accommodation: attempt to compensate for a refractive anomaly. • Occurs when excessive near work is done with bad illumination, bad reading position, state of neurosis, mental stress or anxiety. SPASM OF ACCOMMODATION
- 57. 4/12/2023 57 Clinical features • Defective vision: due to induced myopia. • Asthenopic symptoms • Precipitating factors like marked degree of muscular imbalance, trigeminal neuralgia, a dental lesion, general intoxication. SPASM OF ACCOMMODATION
- 58. 4/12/2023 58 Treatment • Relaxation of ciliary muscle by atropine for 4 weeks or more and • Prohibition of near work allow prompt recovery from spasm of accommodation. • Elimination of the associated causative factors to prevent the recurrence. SPASM OF ACCOMMODATION
- 59. END 4/12/2023 59
Editor's Notes
- Line spacing + Page numbers