M mode sonographic of diaphragmatic motion
•
0 likes•64 views

M-mode sonograpny (US) of the diaphragmatic motion may be an aid for the respiratory therapist to better calibrate the cough-assist machine in uncooperative patients
Recommended

Recommended
More Related Content
Similar to M mode sonographic of diaphragmatic motion
Similar to M mode sonographic of diaphragmatic motion (20)
Recently uploaded
Recently uploaded (20)
M mode sonographic of diaphragmatic motion
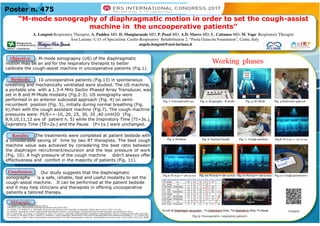
- 1. “M-mode sonography of diaphragmatic motion in order to set the cough-assist machine in the uncooperative patients” A. Longoni Respiratory Therapist, A. Paddeu MD, D. Mangiacasale MD, P. Pozzi MD, A.D. Marco MD, L. Cattaneo MD, M. Vago Respiratory Therapist Asst Lariana -U.O. of Specialistic Cardio-Respiratory Rehabilitation 2, “Paola Giancola Foundation”, Cantù, Italy angelo.longoni@asst-lariana.it M-mode sonograpny (US) of the diaphragmatic motion may be an aid for the respiratory therapist to better calibrate the cough-assist machine in uncooperative patients (Fig.1). 1 G. Soldati, R. Copetti, Ecografia toracica (2012) 2 Winfocus’ Lung ultrasound for anesthesia & intensive care (WLUS-AIC) 3 A. Sarwal, F. O. Walker, M. S. Cartwright, Neuromuscular Ultrasound for evaluation of diaphragm. Muscle Nerve (2013), 47(3): 319-329; 4 A.Zanforlin, Applicazioni cliniche e sperimentali dell’ecografia toracica in pneumologia: la diagnostica precoce delle patologie pleuropolmonari (2012) 5.E. O. Gerscovich, M. Cronan. J. P. McGahan, K. Jain, C. D. Jones, C. McDonald, Ultrasonographic evaluation of diaphragmatic motion. J Ultrasound Med (2001) 597-604; 6 G. Ferrari, G. De Filippi, F. Elia, F. Panero, G. Volpicelly, F. Aprà, Diaphragm ultrasound as a new index of discontinuation from mechanical ventilation. C. U. J. (2014) 6:8 7 A. Boussuges, Y. Gole, P. Blanc, Diaphragmatic motion studied by M-mode ultrasonography: Methods, reproducibility and normal values. Chest (2009) 135(2):391-40089 Our study suggests that the diaphragmatic sonography is a safe, reliable, fast and useful modality to set the cough-assist machine. It can be performed at the patient bedside and it may help clinicians and therapists in offering uncooperative patients a tailored therapy. The treatments were completed at patient bedside with a considerable saving of time by two RT therapists. The best cough machine value was achieved by considering the best ratio between the diaphragm recruitment/excursion and the less pressure of work (Fig. 10). A high pressure of the cough machine didn’t always offer effectiveness and comfort in the majority of patients (Fig. 11). 10 uncooperative patients (Fig.13) in spontaneous breathing and mechanically ventilated were studied. The US machine, a portable one with a 1.3-4 MHz Sector Phased Array Transducer, was set in B and M-Mode modality (Fig.2-3). US sonography were performed in an anterior subcostal approach (Fig. 4) on semi- recumbent position (Fig. 5), initially during normal breathing (Fig. 6),then with the cough assistant machine (Fig.7). The cough machine pressures were: PI/E=+-10, 20, 25, 30, 35 ,40 cmH2O (Fig . 8,9,10,11,12 are of patient n. 5) while the Inspiratory Time (TI=3s.), Expiratory Time (TE=2s.) and the Pause (P=1s.) were unchanged. Poster n. 475 Objective: Methods: Results: Working phases Fig. 1: Uncooperative pz. Fig. 2: Ecography –B mode Fig. 3: M-Mode Fig. 4:Subcostal approch Fig.9: Pz n.5=+- 20 cm H2O Fig. 10: Pz n.5=+- 30 cm H2O Fig. 11: Pz n.5=+- 40 cm H2O Fig.12: Cough parameters Fig.13: Uncooperative respiratory patient’s Fig. 5 :Position Fig. 6: Normal breath Fig. 7: Cough machine Fig.8: Pz n.5=+- 10 cm H2O Conclusion: Contacts Bibliography: