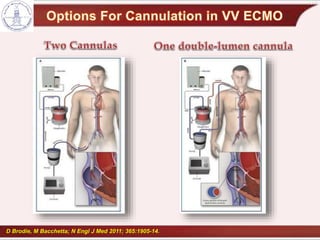
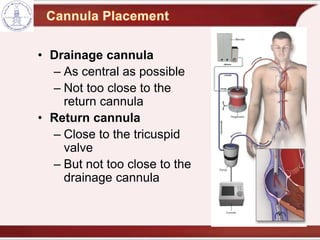
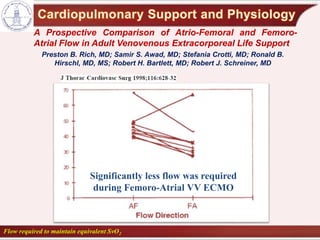
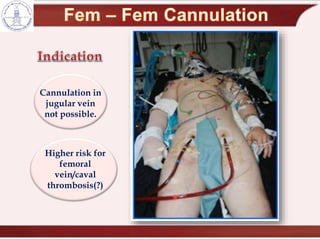
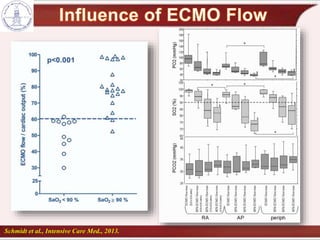
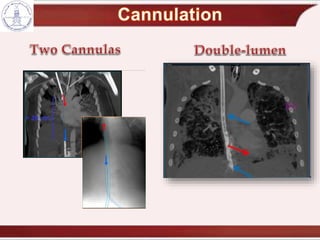
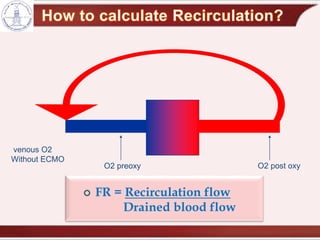
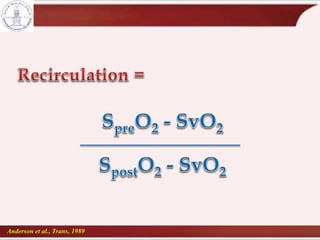
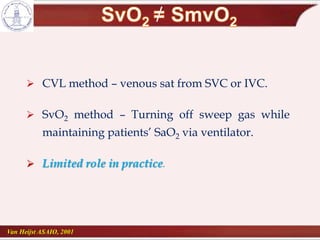
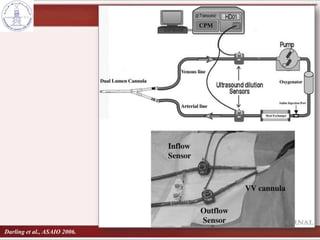
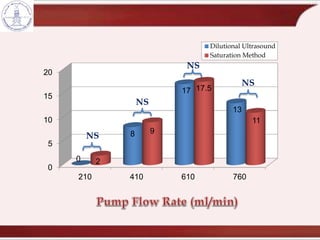
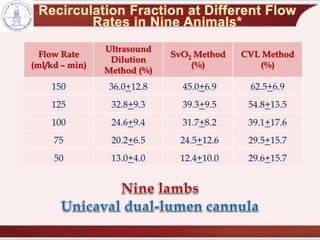
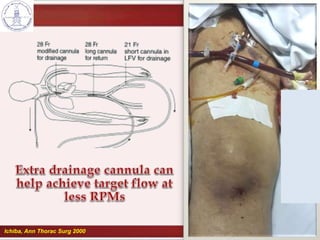
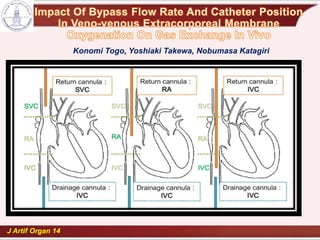
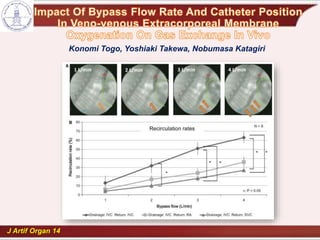
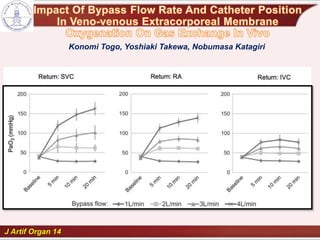
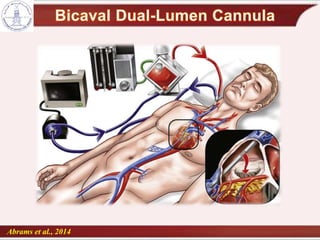
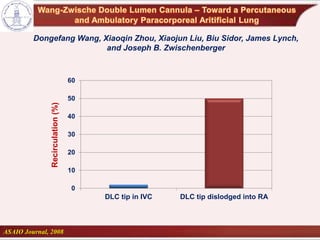
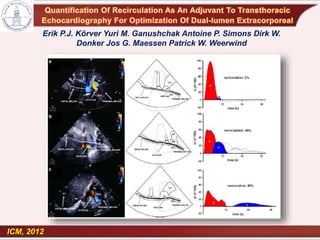
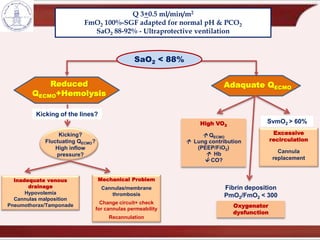
This document discusses various aspects of venovenous extracorporeal membrane oxygenation (VV ECMO) cannulation and management. It provides details on different cannulation strategies and their effects on recirculation. Specifically, it notes that femoro-atrial cannulation had significantly less flow requirement compared to atrio-femoral cannulation during VV ECMO. It also discusses techniques to minimize recirculation like using larger dual-lumen cannulae and ultrasound guidance for proper cannula positioning. Monitoring recirculation is important to optimize ECMO efficiency and outcomes.