Calcium Pyrophosphate Dihydrate Deposition Disease (CPPD), also known as pseudogout, is defined by arthritis with evidence of calcium pyrophosphate dihydrate (CPPD) crystal deposition in cartilage and surrounding tissues. CPPD crystals appear as weakly birefringent rhomboid or rod shapes under polarized microscopy. CPPD typically presents in older adults and can manifest as asymptomatic deposition, acute self-limiting arthritis flares, or chronic inflammatory arthritis. Radiography may reveal chondrocalcinosis, osteoarthritis-like changes in unusual joints, and cysts. Treatment involves lifestyle modifications, medications like NSAIDs to manage symptoms, and arthrocentesis for severe flares.
Introduction
• Calcium pyrophosphatedihydrate disease (CPPD) is also known
as pyrophosphate arthropathy or pseudogout.
• Is defined by the co-occurrence of arthritis with evidence of CPPD
deposition within the articular cartilage.
• CPPD crystals are deposited in articular + surrounding tissues
(bursae, tendon sheaths and the annulus of the intervertebral
discs).
3
4.
Epidemiology
• The estimatedincidence is around 1:250,000-1,000,000.
• Usually in 5th decade of life or older, with increasing
prevalence as age increases.
• Male and female are equally affected.
4
5.
Pathology
• The crystalsare weakly positively birefringent on polarized
microscopy and have a rhomboid or rod shape (cf. to
negatively birefringent needle shaped crystals in gout).
5
6.
Aetiology
• Causes ofCPPD can be divided into:
• Idiopathic
• Hereditary : AD pattern; mutation in the ANKH gene which
encodes a transmembrane inorganic pyrophosphate
transporter.
• Secondary: associated with hemochromatosis,
hyperparathyroidism, hypothyroidism, hypomagnesemia,
previous joint injury, ochronosis.
6
7.
Clinical Presentation
• CPPD:occurrence of calcium pyrophosphate crystals, with or
without symptoms
• Asymptomatic CPPD: chondrocalcinosis +/- changes of
osteoarthritis, but clinically asymptomatic
• Acute CPPD crystal arthritis (formerly pseudogout): self-
limiting synovitis in the setting of CPPD
• Osteoarthritis with CPPD: typical changes
of osteoarthritis in the setting of CPPD
• Chronic CPPD crystal inflammatory arthritis
7
Radiologic Features: PlainRadiography
• Chondrocalcinosis
- Classically occurs in the hyaline and fibrocartilage structures
of the knee and wrist but can be seen in all joints.
- Appears as crystal deposit (opacities of calcific density).
9
10.
Radiologic Features: PlainRadiography
• Osteoarthritis-like pattern
- Narrowed joint space + subchondral sclerosis + subchondral cyst.
- Unusual distribution : non-weight bearing joint (IC and MCP joints)
and symmetrical
- Predilection for the patellofemoral compartment in the knee and the
radiocarpal compartment in the wrist.
- Erosion is not a feature of CPPD arthropathy, though remodelling of
the femoral aspect of the patellofemoral joint is well recognised.
20
11.
Radiologic Features: PlainRadiography
• Hands
- Distribution: 1 CMC; 2nd + 3rd MCP joints; bilateral symmetric
- Resembling degenerative joint disease (without DIP and PIP
involvement)
- Small hook-like osteophytes at radial aspect of metacarpal heads 2
& 3
11
12.
12
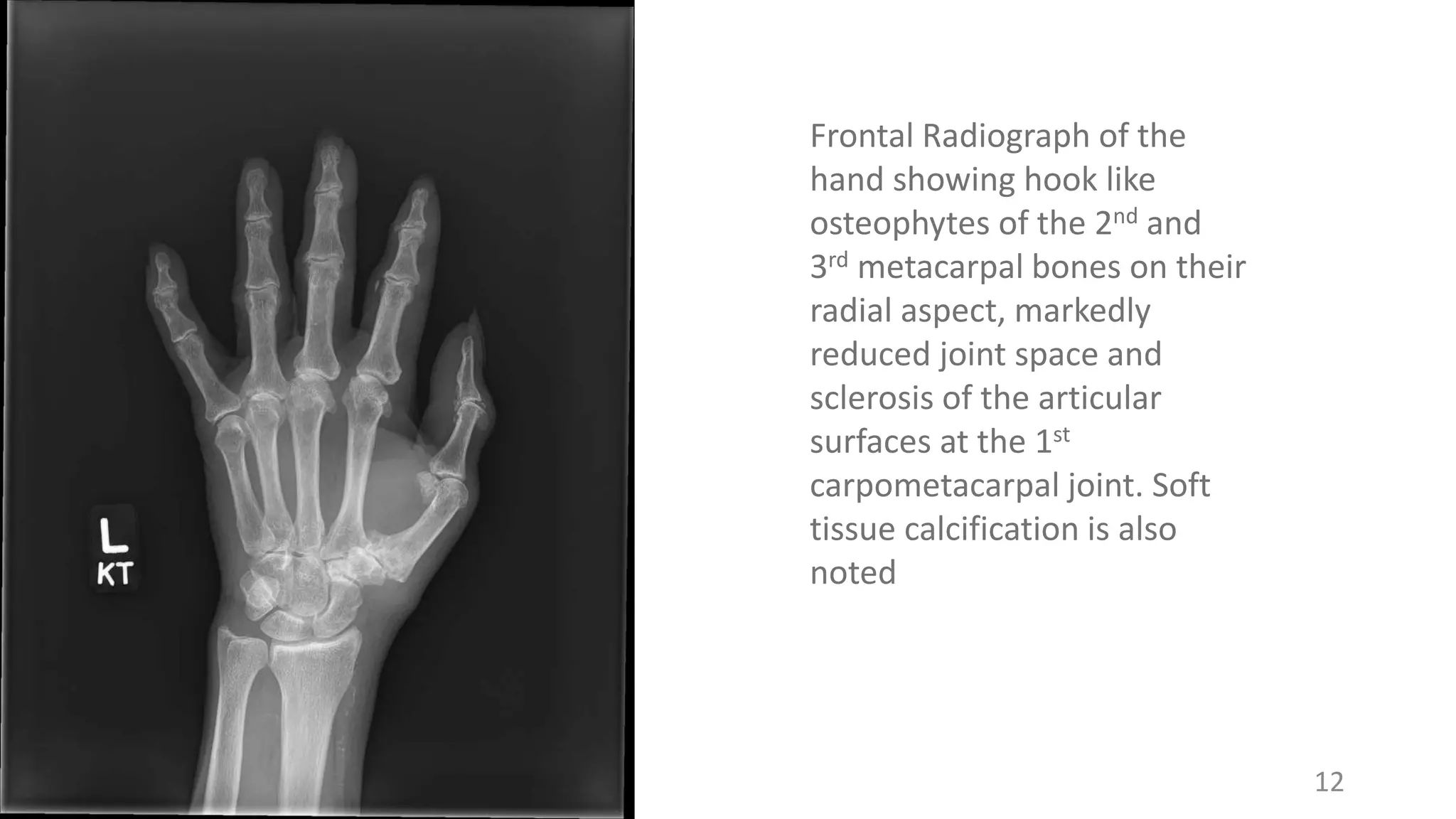
Frontal Radiograph ofthe
hand showing hook like
osteophytes of the 2nd and
3rd metacarpal bones on their
radial aspect, markedly
reduced joint space and
sclerosis of the articular
surfaces at the 1st
carpometacarpal joint. Soft
tissue calcification is also
noted
13.
Radiologic Features: PlainRadiography
• Wrist
- Distribution: triangular fibrocartilage in distal radioulnar joints
bilaterally, proximal carpal row joints at lunotriquetral + scapholunate
ligaments
- Calcification (chondrocalcinosis) of triangular fibrocartilage
- Extensive narrowing / obliteration of joint space between distal radius +
scaphoid → destruction of trapezioscaphoid space:
- Incorporation of scaphoid into articular surface of radius.
- Prominent cysts.
- Scapholunate separation (= ligament tear) → scapholunate advanced
collapse (SLAC)
13
14.
14
Right Wrist JointRadiograph, AP and lateral
views. It shows obliteration of the joint space
between the distal radius and the scaphoid
with sclerosis of their articular surface. There
is a well defined round lytic lesion with thin
sclerotic margins seen in the scaphoid bone
in keeping with subchondral cyst. The
scaphoid and lunate carpal bones also appear
separated. In absence of the history of
trauma, CPPD is favoured as possible
diagnosis.
15.
Radiologic Features: PlainRadiography
• Knee
- Distribution: especially meniscus + cartilage of patellofemoral joint.
- Medial femorotibial + patellofemoral compartments commonly
involved simultaneously (as in osteoarthritis) but with greater
osseous destruction + fragmentation.
- Scalloping of the anterior femoral cortex at the level of the patella.
- Disproportionate narrowing of patellofemoral joint.
15
16.
16
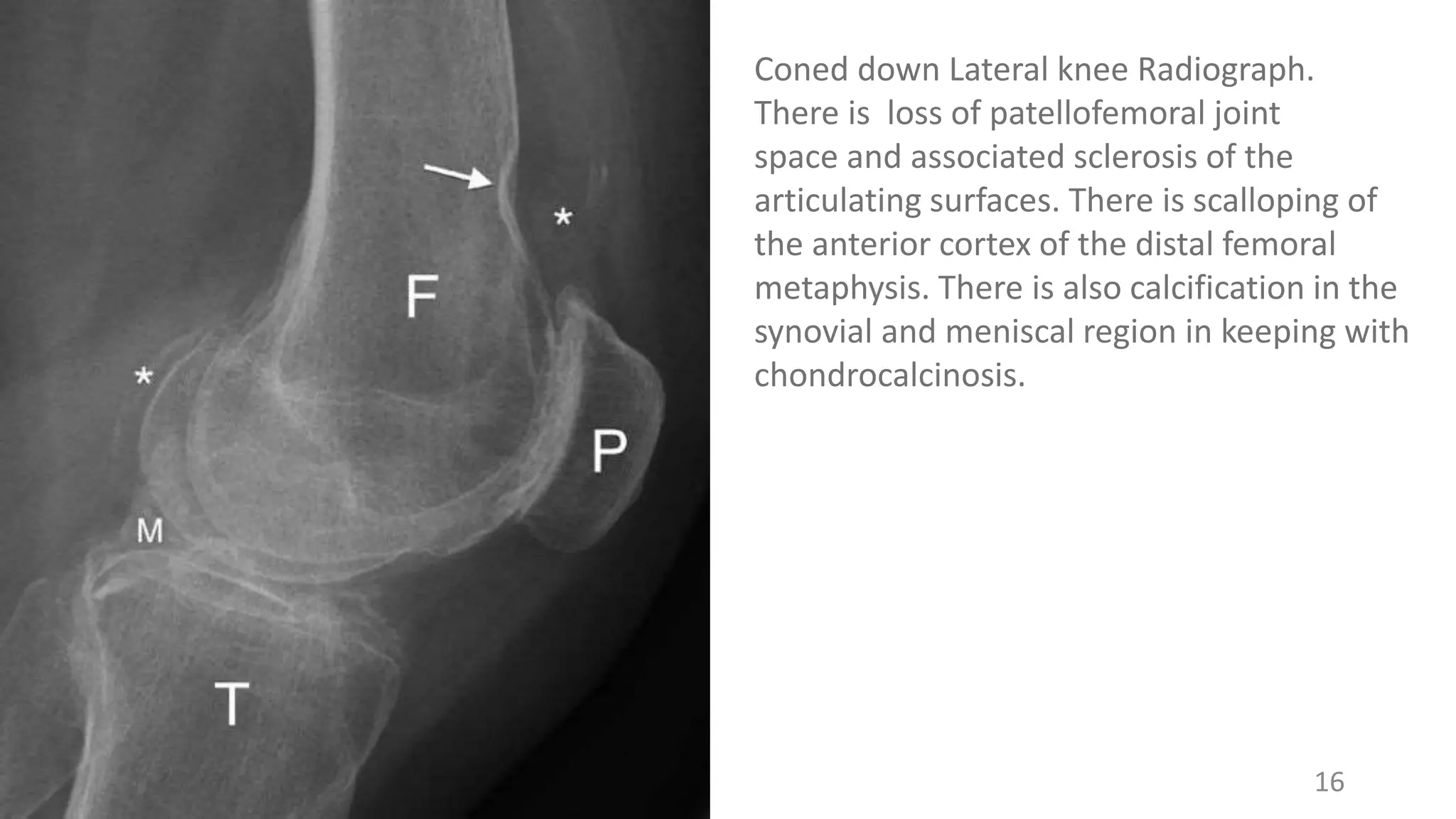
Coned down Lateralknee Radiograph.
There is loss of patellofemoral joint
space and associated sclerosis of the
articulating surfaces. There is scalloping of
the anterior cortex of the distal femoral
metaphysis. There is also calcification in the
synovial and meniscal region in keeping with
chondrocalcinosis.
17.
Radiologic Features: PlainRadiography
• Spine
- Chondrocalcinosis / calcifications of outer fibres of annulus fibrosus of
(lumbar) spine resembling syndesmophytes; NEVER in nucleus pulposus.
- Crowned dens syndrome: periodontal calcification (above and sides of the
top of the dens).
- DDx: Ochronosis (in nucleus pulposus).
• Other Locations
- Pelvis (sacroiliac joint, symphysis): vertical radio opaque line in symphysis
pubis
- Shoulder (glenoid), hip (labrum), elbow, ankle, acromioclavicular joint
17
18.
18
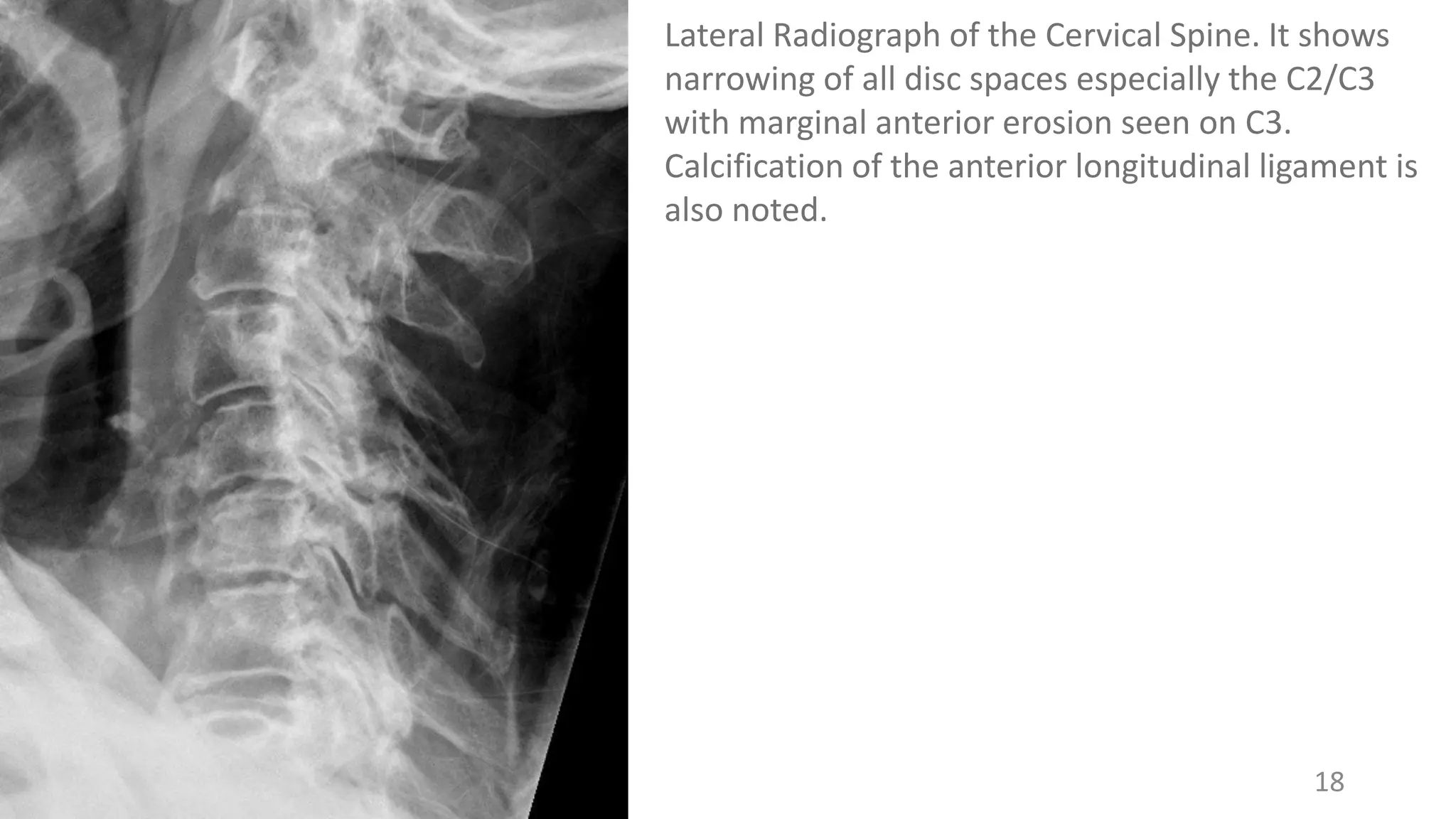
Lateral Radiograph ofthe Cervical Spine. It shows
narrowing of all disc spaces especially the C2/C3
with marginal anterior erosion seen on C3.
Calcification of the anterior longitudinal ligament is
also noted.
19.
Radiologic Features: Ultrasonography
•Synovitis: hypoechoic synovial thickening with increased
vascularity on colour or power doppler.
• Degree of abnormal blood flow proportional to severity of
clinical manifestation.
• CPPD calcifications/deposits: Echogenic materials located
within the articular cartilage itself(cf. to gout’s surface of
articular cartilage) and other surrounding tissues.
19
20.
20
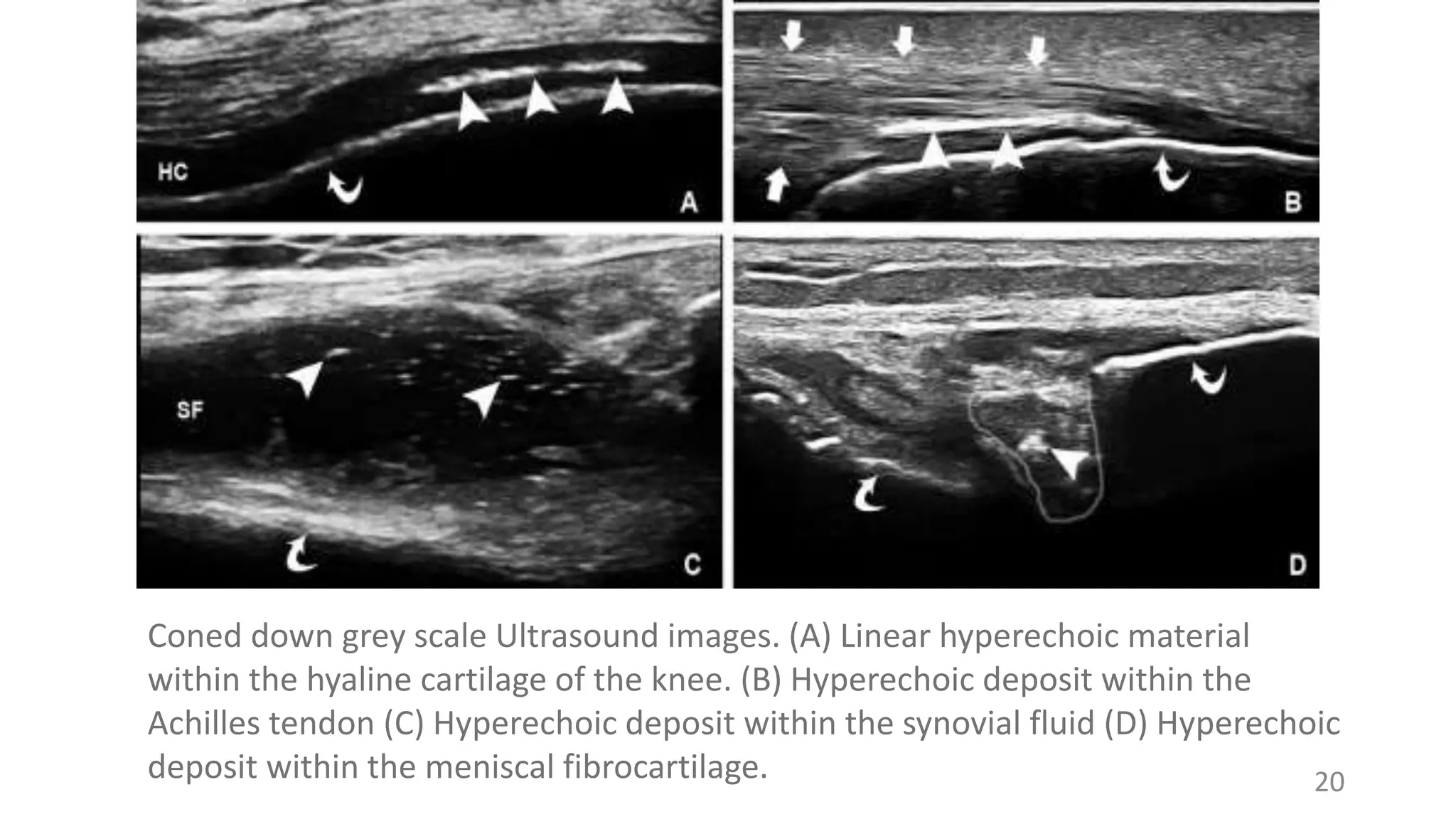
Coned down greyscale Ultrasound images. (A) Linear hyperechoic material
within the hyaline cartilage of the knee. (B) Hyperechoic deposit within the
Achilles tendon (C) Hyperechoic deposit within the synovial fluid (D) Hyperechoic
deposit within the meniscal fibrocartilage.
21.
Radiologic Features: CT
•May show hyperdense mass (of calcific density) with lobulated
configuration and septum-like hypodense areas within it typically
seen in the ligamentum flavum or within joint capsule.
• Others features that may be seen are:
• Fine granular calcification
• Subchondral cyst as well as fracture
• Crowned dens syndrome (CT gold standard)
• Routine x-rays usually reveals CPPD more accurately.
Breakdown of prosthesis can mimic CPPD.
21
22.
22
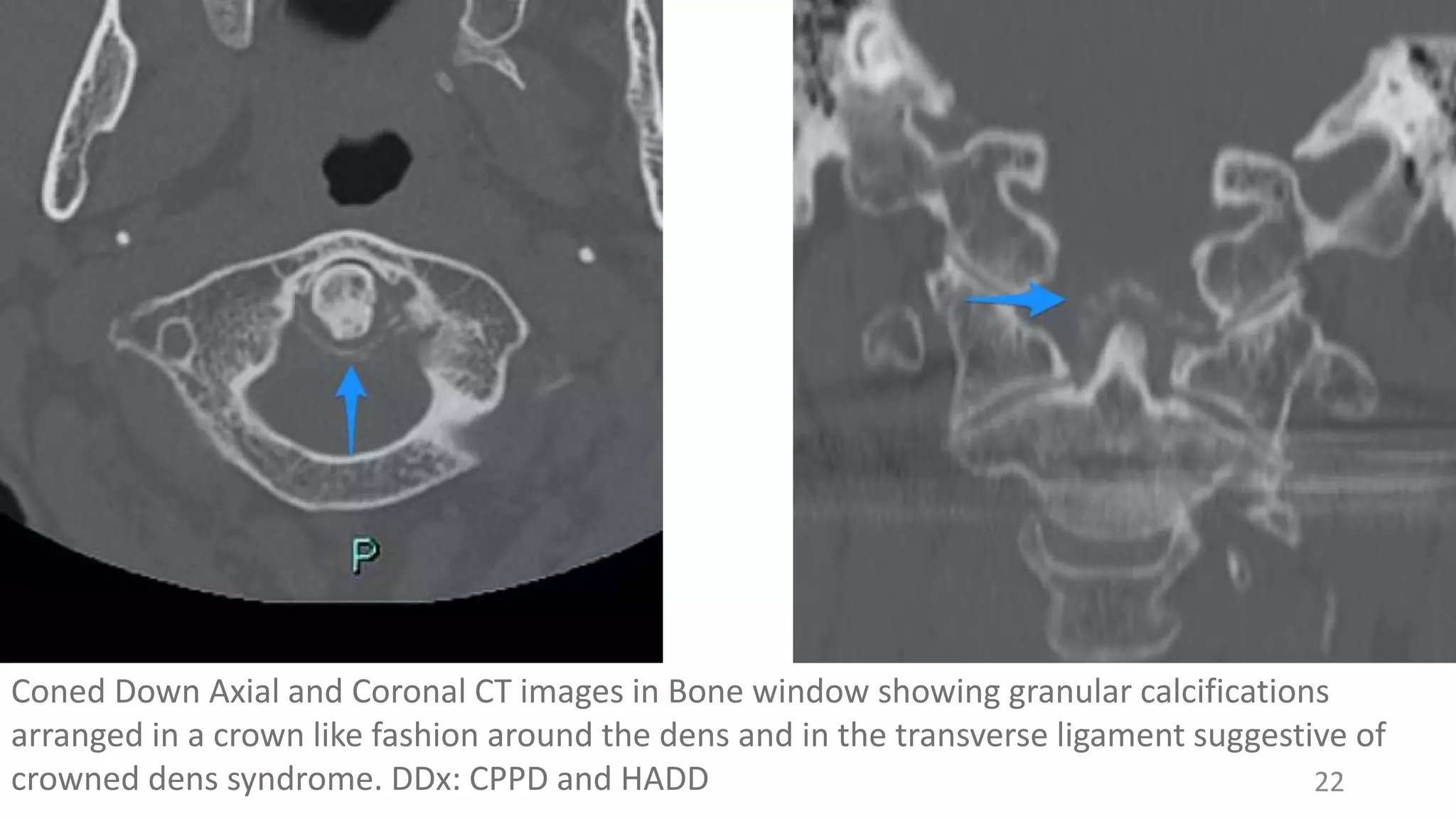
Coned Down Axialand Coronal CT images in Bone window showing granular calcifications
arranged in a crown like fashion around the dens and in the transverse ligament suggestive of
crowned dens syndrome. DDx: CPPD and HADD
23.
Radiologic Features: MRI
•T1-weighted
- Low-signal intensity with punctate signal void
• T2-weighted
- Varying signal intensity
- Rim enhancement rarely noted
• T1-weighted + Gad
- Peripheral enhancement
• Assoc. fracture: low intensity line on T1, T2 weighted spin echo.
• Findings can mimic prosthetic joint breakdown and meniscal tear.
23
24.
24
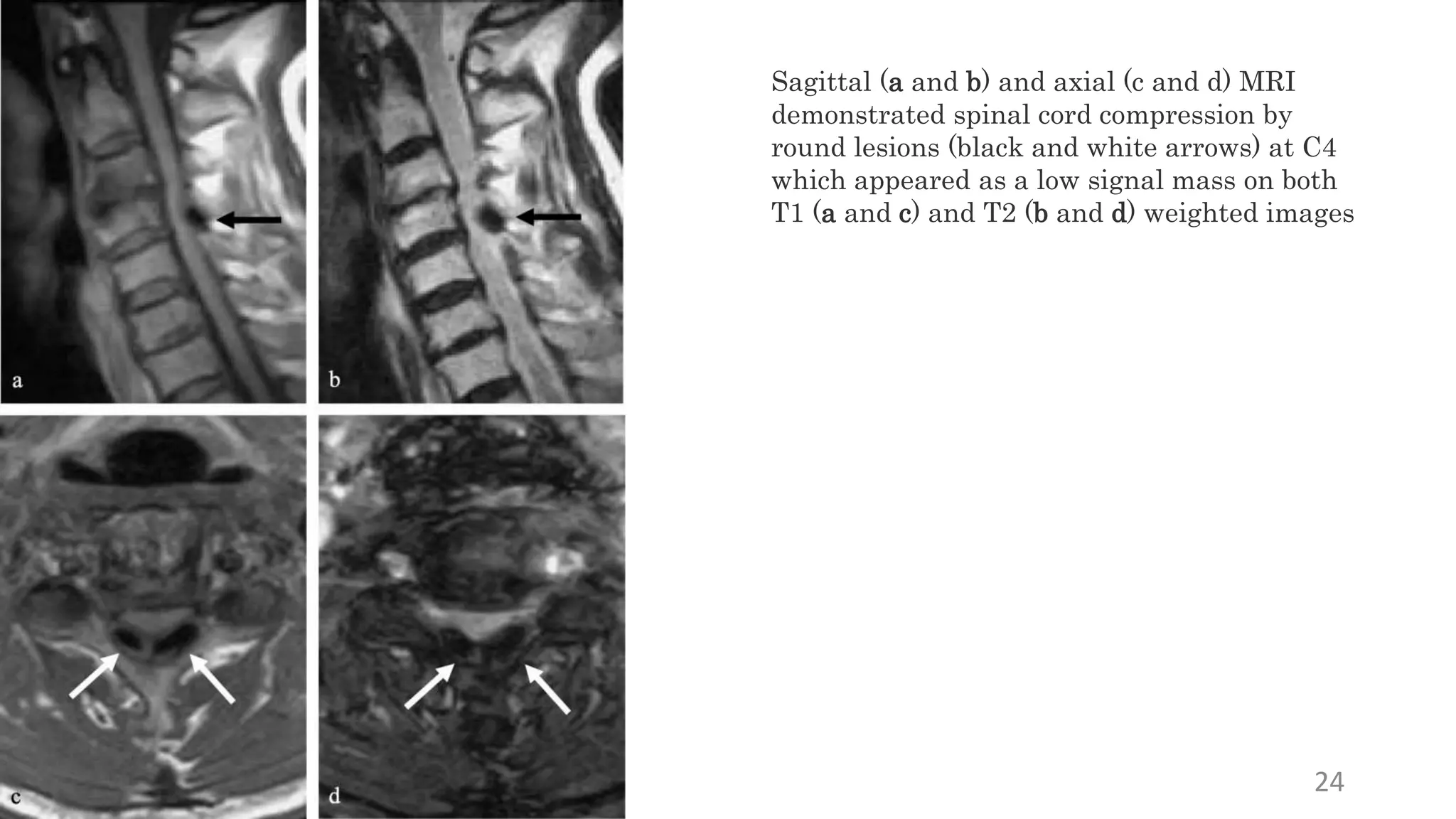
Sagittal (a andb) and axial (c and d) MRI
demonstrated spinal cord compression by
round lesions (black and white arrows) at C4
which appeared as a low signal mass on both
T1 (a and c) and T2 (b and d) weighted images
25.
Radiologic Features: NuclearImaging
• Increased uptake of bone-seeking radiopharmaceuticals
(99mTc-labelled disphosponate) in affected joints.
• Extraosseous calcific deposits may also show increase
uptake.
• Highly sensitive but no specific: localized tissue hyperemia,
recent joint trauma or surgery, arthritis of any cause can
produce identical results.
25
26.
Differential Diagnosis
• Gout:periarticular crystal deposited cf. to intra-articular
deposition in CPPD. Affects lower limb, typically 1st
metatarsophalangeal joint. Causes bony erosion.
• Calcium Hydroxyapatite Deposition Disease (HADD): also
periarticular crystal deposited cf. to intra-articular
deposition in CPPD. Affect shoulder mostly.
• Osteoarthritis: usually have the typical weight-bearing
distribution.
• Giant Cell Tumour (GCT): subchondral cysts of CPPD can be
large and simulate subchondral GCT
26
27.
Treatment
• Depends onclinical manifestation
• Asymptomatic: no treatment
- If asymptomatic + secondary cause: treat underlying condition.
• Symptomatic
- Lifestyle: Ice packs
- Medications: NSAIDs, steroids (intra-articular, systemic),
Colchicine, Intra-articular Na hyaluronate, Hydroxychloroquine
(prevent flareup)
- Medical procedure: arthrocentesis
• Prognosis
-Outcome is generally good, aggressive treatment can lead to
complete resolution.
27