Downloaded 85 times



![Laboratory diagnosis
Serologic testing
For yeast and mycelial antigens
Complement Fixation more sensitive [>1:8 in 90%
of acute pulmonary cases; immunodiffusion more
specific [76% M band +, 23% H band +]
Develop 2 to 6 weeks after infection
May be elevated from past or asymptomatic
infection
Low titer or false negative if immunocompromised](https://image.slidesharecdn.com/4-english-histo060217bke-170606150934/85/Overview-of-Histoplasmosis-41-320.jpg)
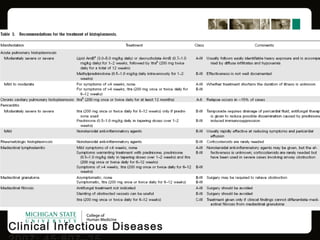


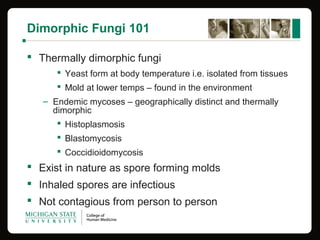
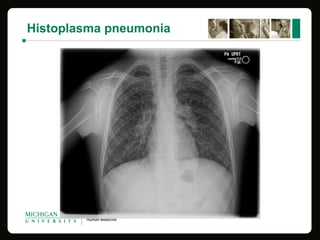
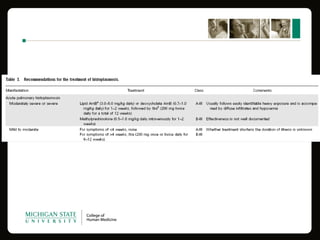
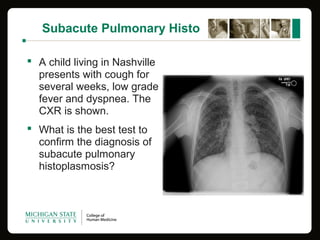
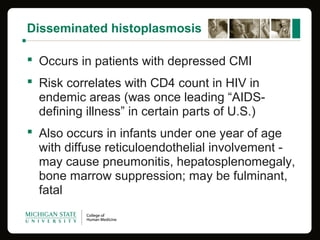
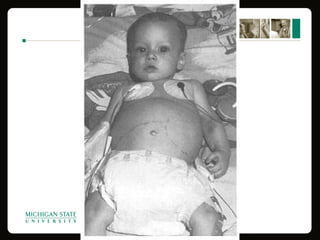
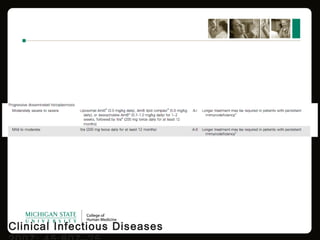
This document provides an overview of histoplasmosis, including its epidemiology, pathophysiology, clinical manifestations, diagnosis, and treatment. It describes how histoplasmosis is caused by the dimorphic fungus Histoplasma capsulatum, which exists as a mold in the environment and a yeast in tissues. Most infections are asymptomatic, but symptomatic cases can range from mild acute pulmonary infection to potentially fatal disseminated infection. Diagnosis involves antigen detection, culture, histopathology, or serologic testing. Treatment with antifungals is recommended for severe or disseminated cases.























































































