Downloaded 239 times
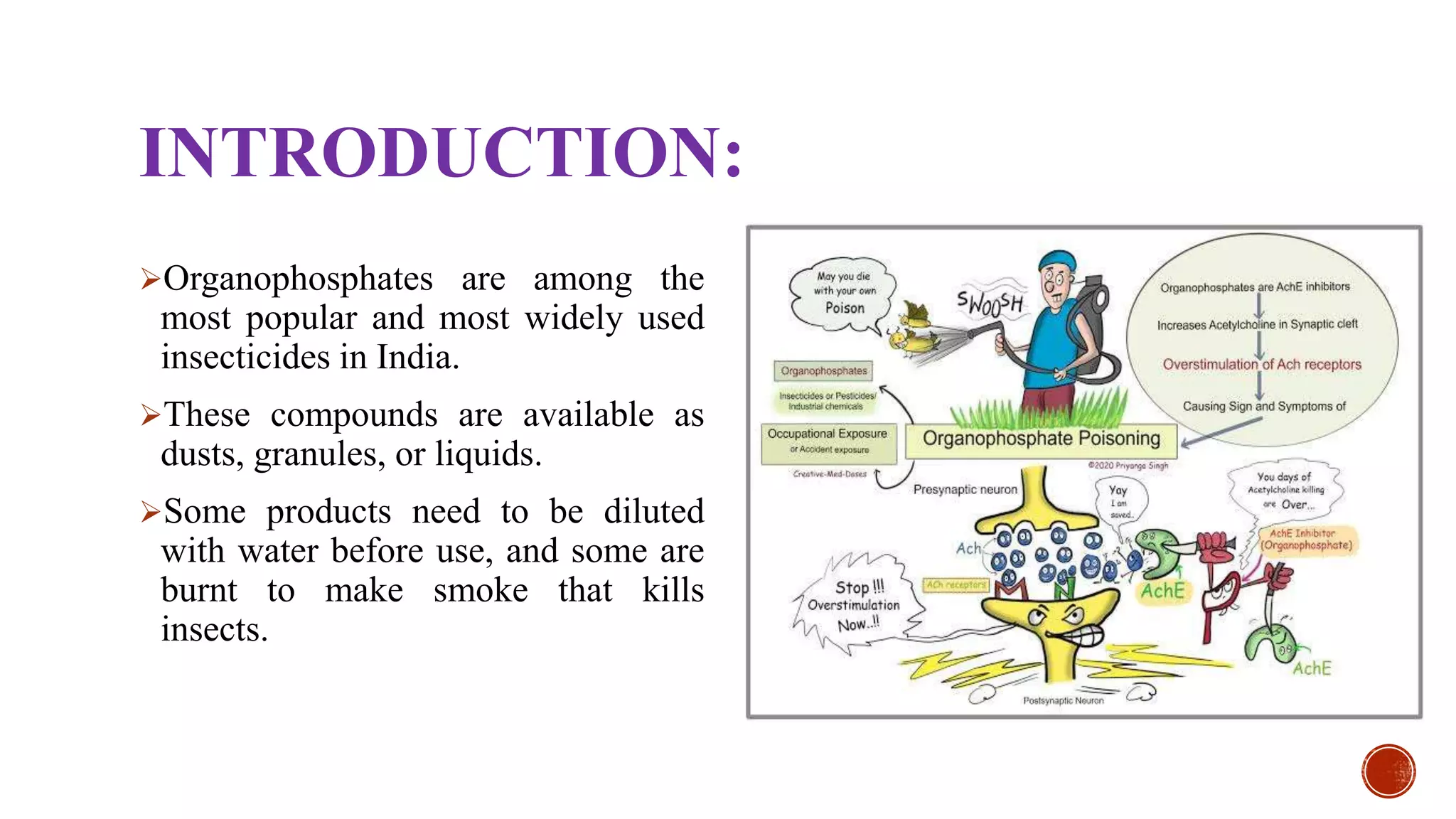
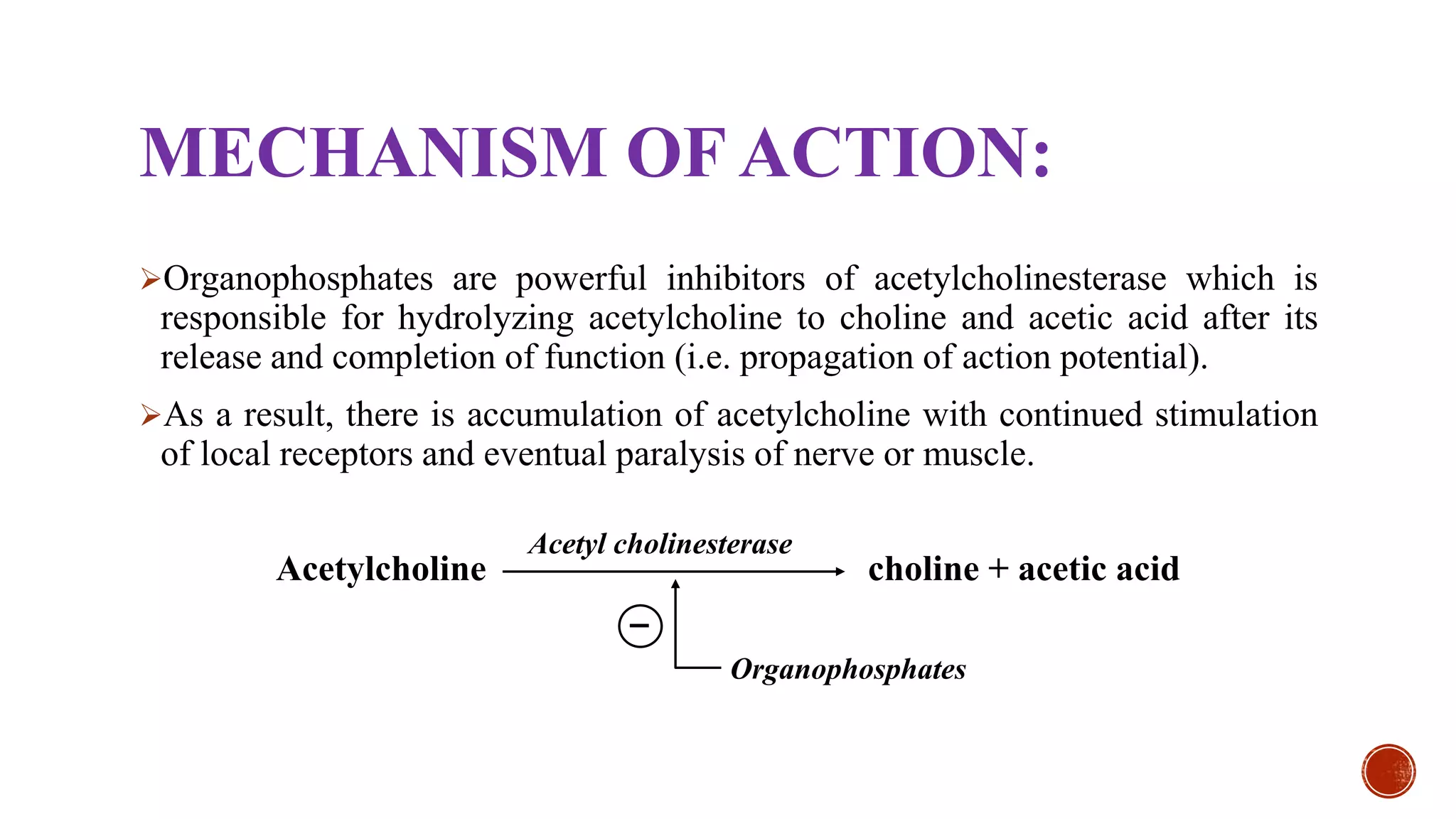
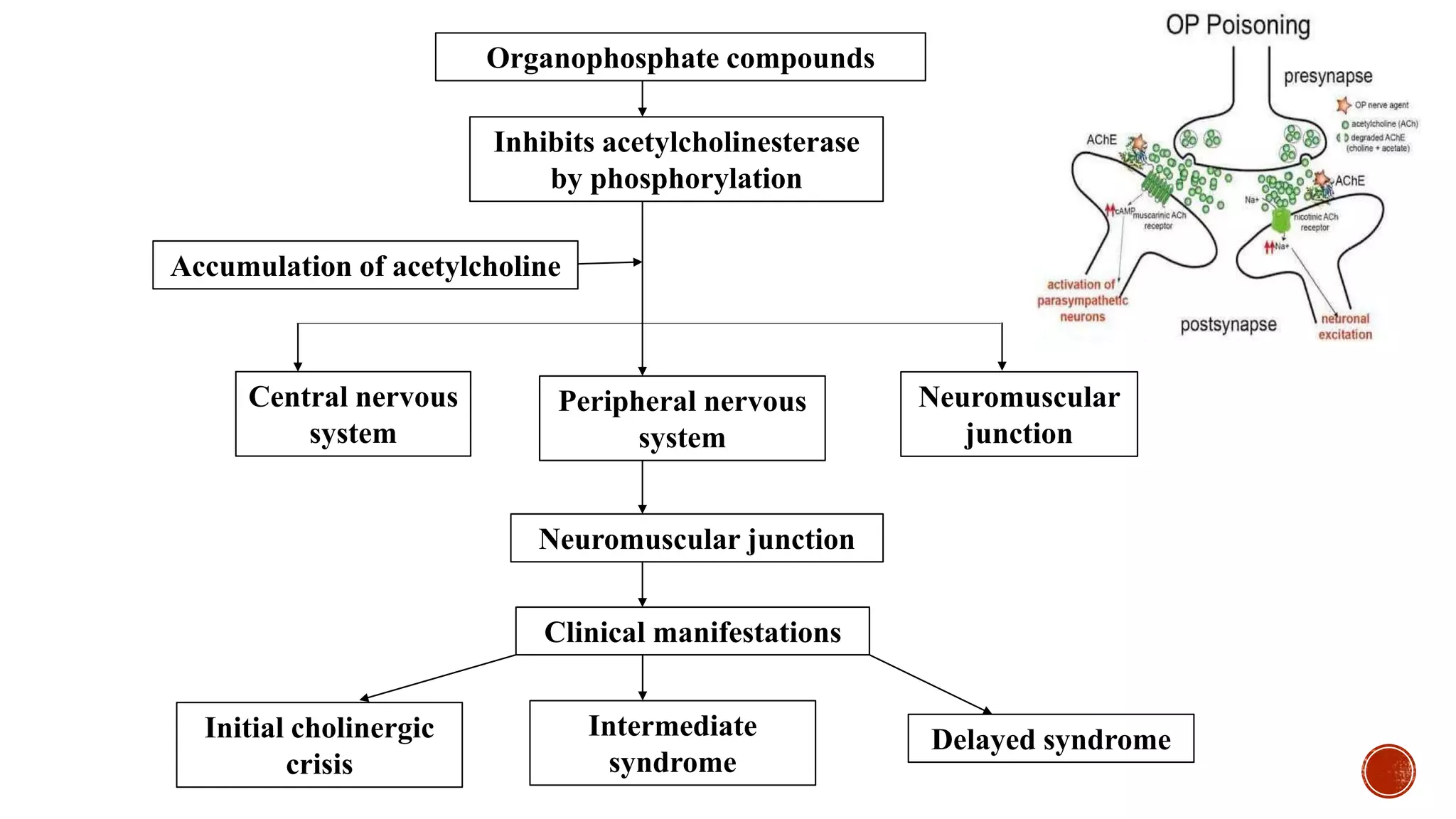











The document details organophosphate poisoning, including its introduction, usual fatal doses, mechanism of action, clinical symptoms, diagnosis, and management. Organophosphates inhibit acetylcholinesterase, leading to acetylcholine accumulation and subsequent toxicity, with management including decontamination, antidotes like atropine and pralidoxime, and supportive measures. Chronic poisoning occurs primarily in agricultural workers, necessitating removal from exposure and supportive care.