Download as PDF, PPTX

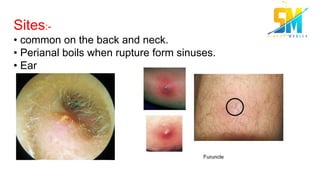



Folliculitis is an infection and inflammation of one or more hair follicles that can occur anywhere on the skin except the palms and soles. It has infectious causes like Staphylococcus aureus and non-infectious causes such as chemicals or mechanical irritation. Treatment depends on the cause and severity but includes topical or oral antibiotics. Boils are infections of a single hair follicle by S. aureus that appear as painful swellings, while carbuncles are larger aggregations of interconnected boils involving deeper tissue. Both require incision, drainage and systemic antibiotics.



































































