Bronchial asthama

BRONCHIAL ASTHMA ntroduction Definition Etiological factors Pathophysiology Types of asthma Clinical manifestation Restlessness Wheezing or crackles Absent or diminished lung sounds Hyper resonance Use of accessory muscles for breathing Tachypnea with hyperventilation Clinical manifestation Diagnostic evaluation Bronchoprovocation Testing: Testing that is done to identify inhaled allergens; mucous membranes are directly exposed to suspected allergen in increasing amounts. Skin Testing: Done to identify specific allergens. Exercise Challenges: Exercise is used to identify the occurrence of exercise-induced bronchospasm. Radio allergosorbent Test: Blood test used to identify a specific allergen. Chest Radiograph: May show hyper expansion of the airways. Managemnet Goal- Promote bronchodilationn Reduce inflammation Remove secretions Prevent ongoing symptoms Prevent asthma attack Maintain normal lung function Avoid triggers Pharmacological therapy 1. Long term control medication- Inhaled corticosteroid Leukotriene modifiers Long acting beta agonist Methylxanthines Combine inhaler 2 Quick relief medication Short acting beta agonist Anticholinergic Oral or I/V corticosteroid 3 Bronchial thermoplasty- Form severe asthma that does not respond to medication Non- pharmacological Oxygen therapy Postural drainage & chest physiotherapy Coughing & deep breathing exercise Avoidance of allergen relaxation technique acupuncture Prevention Patients with recurrent asthma should undergo tests to identify the substances that precipitate the symptoms. Possible causes are dust, dust mites, roaches, certain types of cloth, pets, horses, detergents, soaps, certain foods, molds, and pol- lens. If the attacks are seasonal, pollens can be strongly sus- pected. Patients are instructed to avoid the causative agents whenever possible. Complications Complications of asthma may include status asthmaticus, respiratory failure, pneumonia, and atelectasis. Airway obstruction, particularly during acute asthmatic episodes, often results in hypoxemia, requiring the administration of oxygen and the monitoring of pulse oximetry and arterial blood gases. Fluids are administered, because people with asthma are frequently dehydrated from diaphoresis and in- sensible fluid loss with hyperventilation. Nursing diagnosis Impaired gas exchange r/t altered oxygen supply Ineffective airway clearance r/t bronchospasm & obstruction from narrow lumen Ineffective breathing pattern r/t bronchospasm Risk for increasing attack of r espiratory distress r/t exposure to allergens

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Bronchial asthama
Similar to Bronchial asthama (20)
More from Shyam Bhatewara
Recently uploaded
Recently uploaded (20)
Bronchial asthama
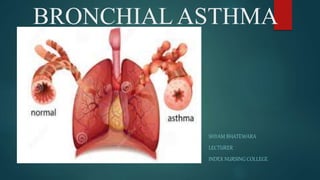
- 1. BRONCHIAL ASTHMA SHYAM BHATEWARA LECTURER INDEX NURSING COLLEGE
- 2. Introduction Asthma is a chronic lung disease that inflames & narrow the airways. Asthma is a reversible, obstructive airway disease in which trachea & bronchi respond in a hyperactive in certain stimuli.
- 3. Definition Chronic inflammatory disorder of the airways that causes varying degrees of obstruction in the airways Marked by airway inflammation and hyper responsiveness to a variety of stimuli or triggers Causes recurrent episodes of wheezing, breathlessness, chest tightness, and coughing associated with airflow obstruction that may resolve spontaneously
- 4. Etiological factors Environmental Factors - Animal Cockroaches Dust Exhaust fumes Fireplaces Molds Perfumes or other products with aerosol sprays Pollen Smoke, including cigarette or cigar smoke Sudden weather changes
- 5. Physiological Factors Gastroesophageal reflux disease (GERD) Hormonal changes Sinusitis Stress Viral upper respiratory infection Genetic factor Hay fever & other allergies
- 6. Medications Acetylsalicylic acid (aspirin) β-Adrenergic blockers Nonsteroidal antiinflammatory drugs Occupational Exposure Factors Metal salts Wood and vegetable dusts Industrial chemicals and plastics
- 7. Pathophysiology Due to etiological factors Reversible and diffuse airway inflammation Hyper responsiveness of airway Airflow limitation Swelling of membrane line of airway Wheezing Cough Contraction bronchial muscle Dyspnea Chest tightness Bronchial enlargement & production of thick cough asthma
- 8. Types of asthma Allergic asthma – induced by hyper-immune response to allergens Non allergic asthma (intrinsic asthma) Mixed asthma- both allergic & non allergic Cough variant asthma- absence of classical symptoms, Only dry cough is present Exercise induced asthma Nocturnal asthma Occupational asthma
- 9. Clinical manifestation Restlessness Wheezing or crackles Absent or diminished lung sounds Hyper resonance Use of accessory muscles for breathing Tachypnea with hyperventilation
- 10. Clinical manifestation Prolonged exhalation Tachycardia Pulsus paradoxus Diaphoresis Cyanosis Decreased oxygen saturation
- 11. Diagnostic evaluation Detailed history collection Pulse oximetry Pulmonary Function Tests: Spirometry testing assesses the presence and degree of disease and can determine the response to treatment. Peak Expiratory Flow Rate Measurement: Measures maxi- mum flow of air that can be forcefully exhaled in 1 second; child uses a peak expiratory flowmeter to determine a “per- sonal best” value that can be used for comparison at other times, such as during and after an asthma attack.
- 12. Diagnostic evaluation Bronchoprovocation Testing: Testing that is done to identify inhaled allergens; mucous membranes are directly exposed to suspected allergen in increasing amounts. Skin Testing: Done to identify specific allergens. Exercise Challenges: Exercise is used to identify the occurrence of exercise-induced bronchospasm. Radio allergosorbent Test: Blood test used to identify a specific allergen. Chest Radiograph: May show hyper expansion of the airways.
- 13. Managemnet Goal- Promote bronchodilationn Reduce inflammation Remove secretions Prevent ongoing symptoms Prevent asthma attack Maintain normal lung function Avoid triggers
- 14. Pharmacological therapy 1. Long term control medication- Inhaled corticosteroid Leukotriene modifiers Long acting beta agonist Methylxanthines Combine inhaler
- 15. 2 Quick relief medication Short acting beta agonist Anticholinergic Oral or I/V corticosteroid 3 Bronchial thermoplasty- Form severe asthma that does not respond to medication
- 17. Non- pharmacological Oxygen therapy Postural drainage & chest physiotherapy Coughing & deep breathing exercise Avoidance of allergen relaxation technique acupuncture
- 18. Prevention Patients with recurrent asthma should undergo tests to identify the substances that precipitate the symptoms. Possible causes are dust, dust mites, roaches, certain types of cloth, pets, horses, detergents, soaps, certain foods, molds, and pol- lens. If the attacks are seasonal, pollens can be strongly sus- pected. Patients are instructed to avoid the causative agents whenever possible.
- 19. Complications Complications of asthma may include status asthmaticus, respiratory failure, pneumonia, and atelectasis. Airway obstruction, particularly during acute asthmatic episodes, often results in hypoxemia, requiring the administration of oxygen and the monitoring of pulse oximetry and arterial blood gases. Fluids are administered, because people with asthma are frequently dehydrated from diaphoresis and in- sensible fluid loss with hyperventilation.
- 20. Nursing diagnosis Impaired gas exchange r/t altered oxygen supply Ineffective airway clearance r/t bronchospasm & obstruction from narrow lumen Ineffective breathing pattern r/t bronchospasm Risk for increasing attack of respiratory distress r/t exposure to allergens