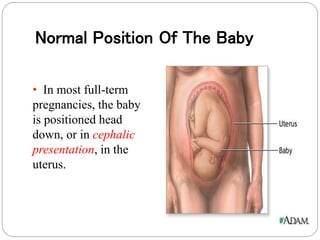
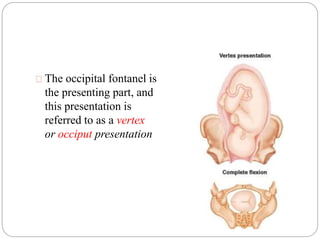
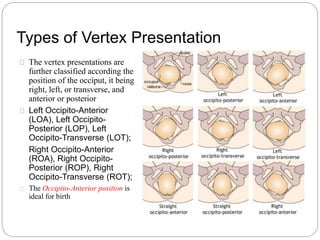
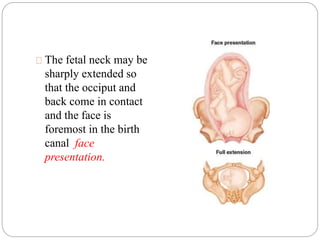
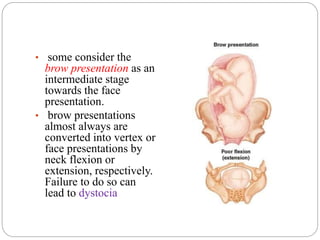
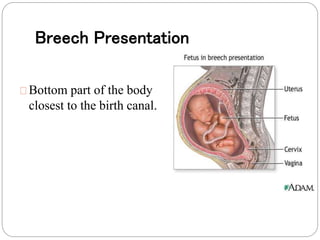
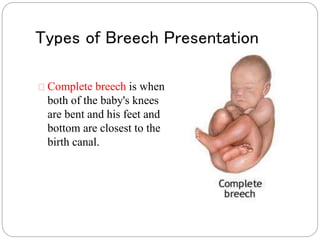
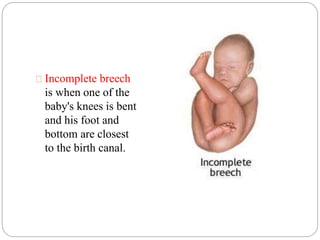
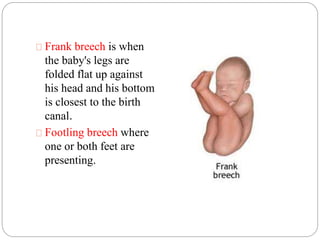
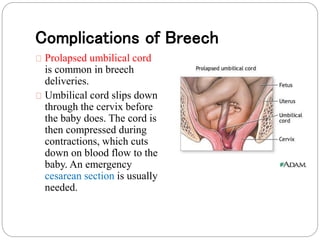
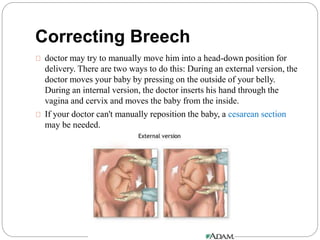
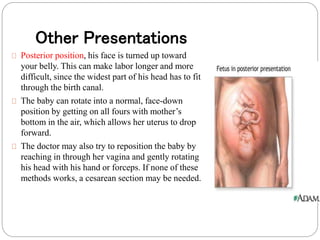
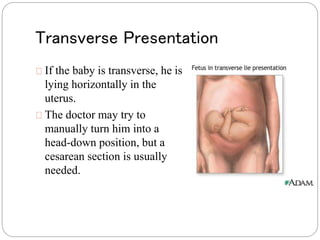
This document discusses fetal presentation during pregnancy and delivery. Fetal presentation refers to the part of the baby's body closest to the birth canal, which can be determined through vaginal exams, ultrasound, or feeling the abdomen. Normally, babies are positioned head down for delivery. Other possible presentations include breech, where the bottom is closest; brow/face, where the forehead or face is closest; and transverse, where the baby lies horizontally. Different presentations carry varying risks and may require techniques like external version to rotate the baby or a cesarean section for delivery.