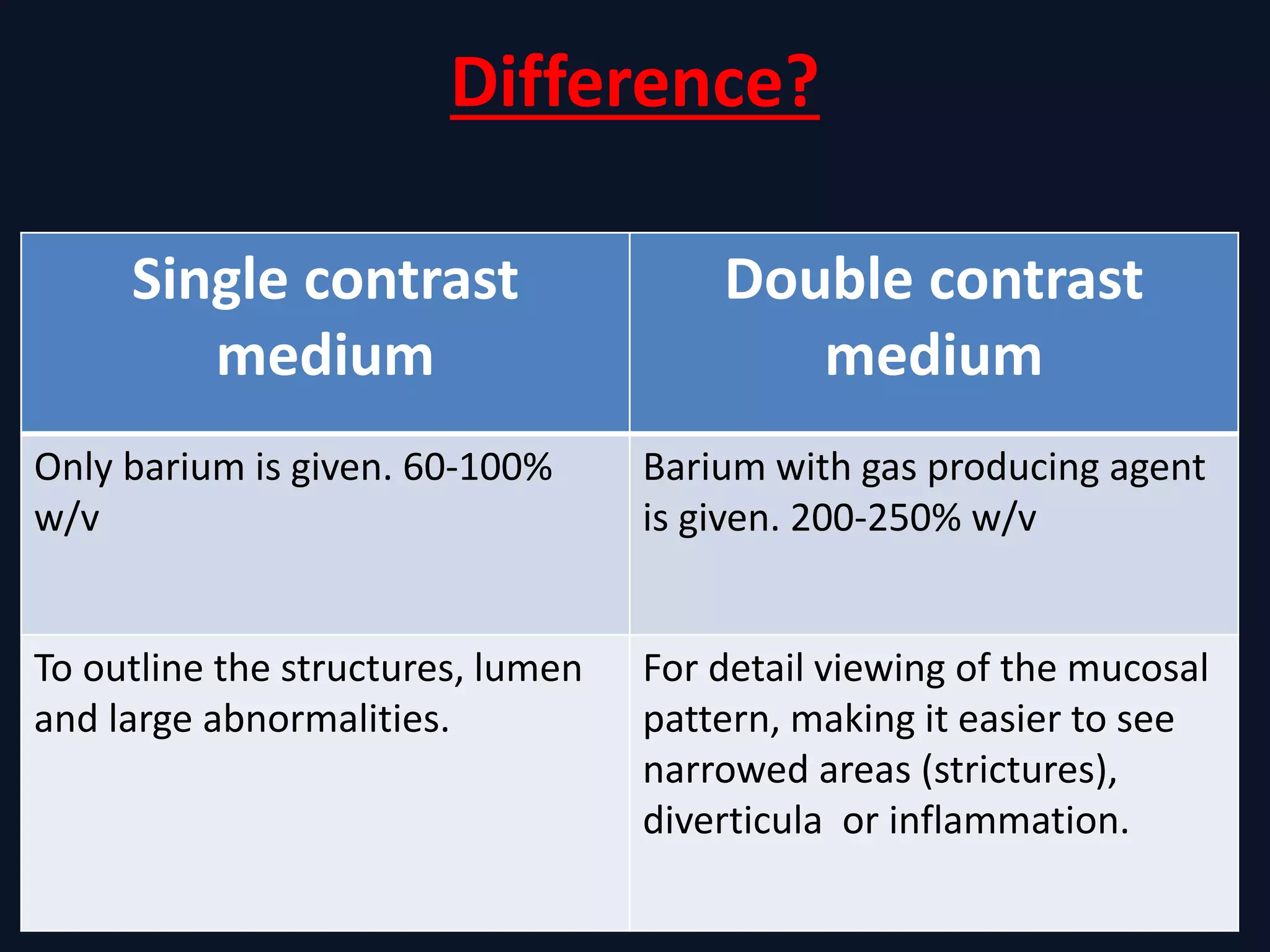
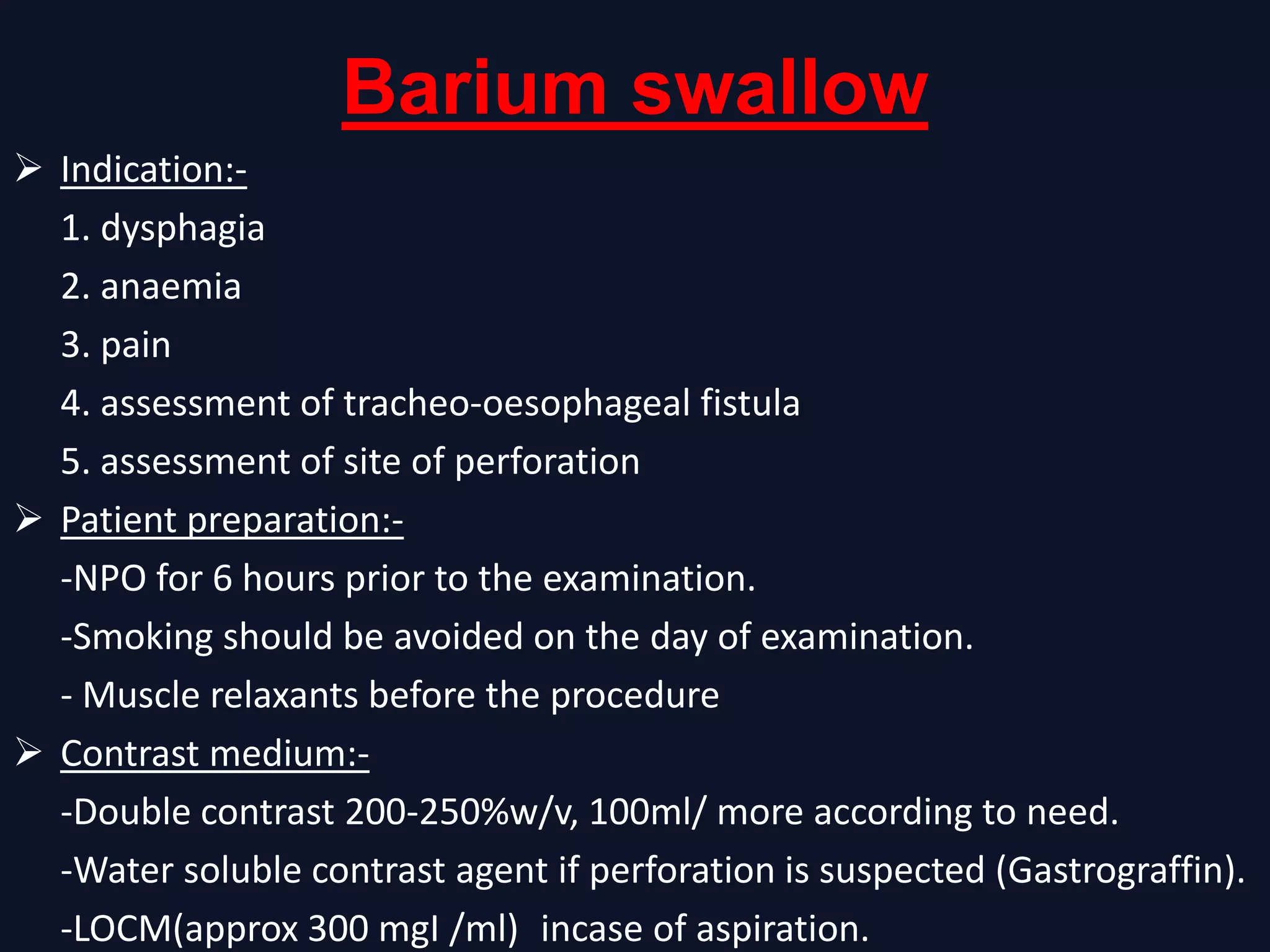
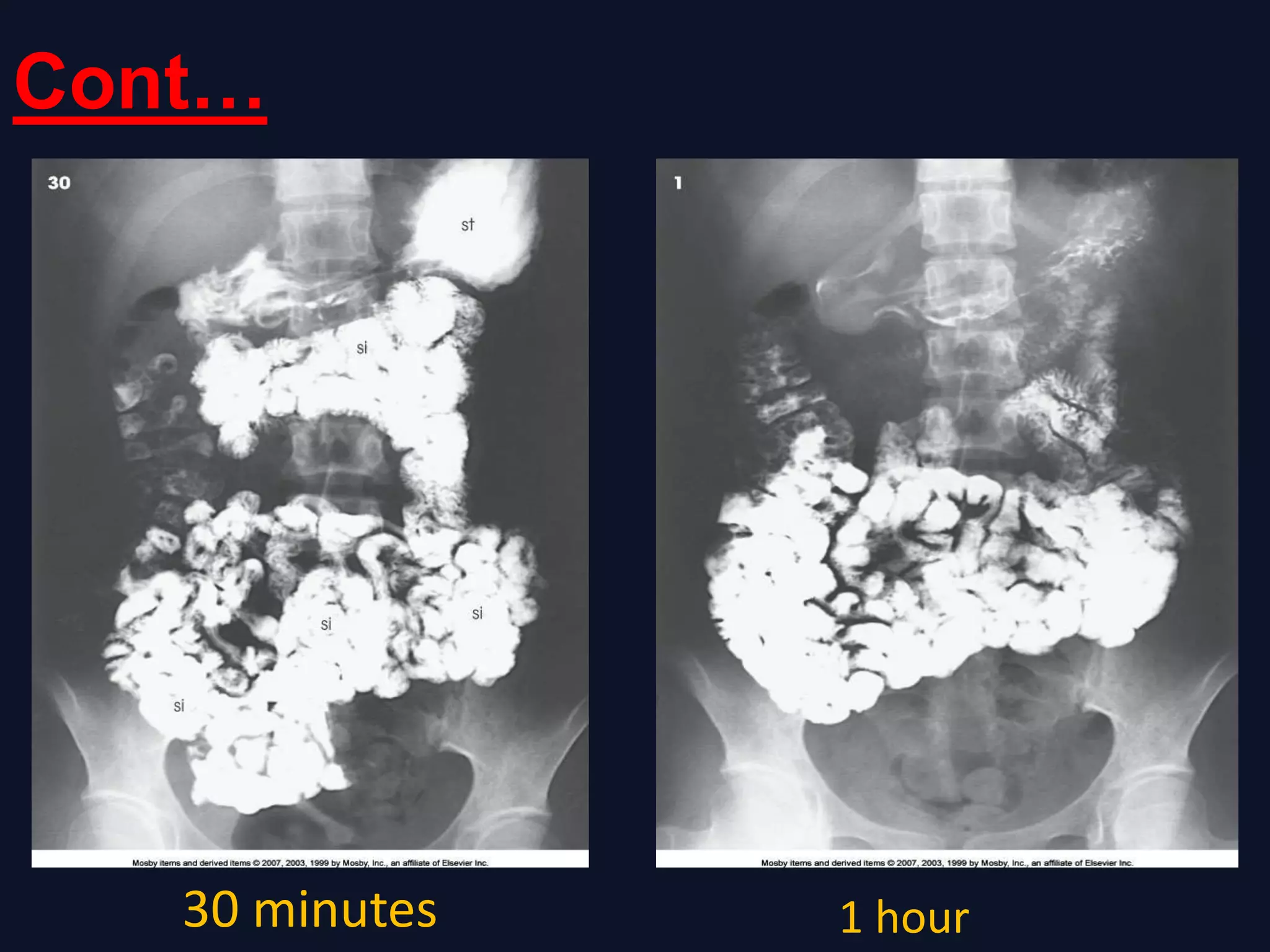
This document provides an overview of gastrointestinal tract imaging procedures using barium as a contrast agent. It describes the characteristics and uses of barium sulfate for outlining GI structures. Various GI imaging techniques are outlined, including barium swallow, barium meal, barium follow through, and barium enema. Patient preparation, contrast agents, positioning, and film techniques are discussed for each procedure. Potential complications are also briefly mentioned.


























![COMPLETE BARIUM STUDIES Of GIT NAD [Adrian Dungu Niyimpa].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/bastudies-gitnad-220902221043-d535eaa3-thumbnail.jpg?width=640&height=640&fit=bounds)
































































