Drugs Used in Endocrine Alteration
•
1 like•667 views

Drugs Used in Endocrine Alteration

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Drugs Used in Endocrine Alteration
Similar to Drugs Used in Endocrine Alteration (20)
More from Subramani Parasuraman
More from Subramani Parasuraman (20)
Recently uploaded
Recently uploaded (20)
Drugs Used in Endocrine Alteration
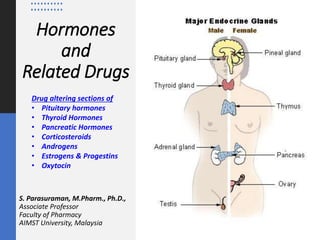
- 1. Hormones and Related Drugs S. Parasuraman, M.Pharm., Ph.D., Associate Professor Faculty of Pharmacy AIMST University, Malaysia Drug altering sections of • Pituitary hormones • Thyroid Hormones • Pancreatic Hormones • Corticosteroids • Androgens • Estrogens & Progestins • Oxytocin
- 2. Pituitary hormones Drug altering the anterior pituitary hormone secretion
- 4. Anterior pituitary hormones Ref: https://labpedia.net/hypothalamus-and-pituitary-gland-hormones/ • Adrenocorticotropic hormone (ACTH): This hormone stimulates the secretion of cortisol by the adrenal gland. • Growth Hormone (GH): This hormone promotes growth in soft tissue, cartilage, and bone. • Thyroid stimulation hormone (TSH): This hormone stimulates the secretion of the thyroid hormone T3 and T4 by the thyroid gland. • Prolactin Hormone (PRL): This hormone’s main role is in the initiation and maintenance of lactation. Prolactin induces ductal growth, the lobular alveolar system, and the synthesis of milk production. • Follicle-stimulating hormone (FSH): This hormone controls the functional activity of gonads. In the male, this stimulates spermatogenesis. In females stimulate the growth of ovarian follicles in the presence of LH. • Luteinizing hormone (LH): This hormone controls the functional activity of the gonads. Males produce testosterone through the Leydig cells of the testes. In females, it leads to the release of the ovum from the ovarian follicle, in which FSH ripens.
- 5. Posterior Pituitary Gland hormones Ref: https://labpedia.net/hypothalamus-and-pituitary-gland-hormones/ • Adrenocorticotropic hormone (ACTH): This hormone stimulates the secretion of Antidiuretic Hormone (ADH). This maintains water homeostasis. This also leads to vasoconstriction to increase blood pressure. • Oxytocin: This will stimulate uterine contraction during labor. This may be used to induce labor. It helps in milk release from the mammary ducts.
- 6. Drug altering the anterior pituitary hormone secretion
- 7. Thyroid Hormones Drug altering the thyroid hormones secretion
- 8. Thyroid Hormones and Thyroid Inhibitors • The thyroid gland secretes 3 hormones - thyroxine (T4), triiodothyronine (T3) and calcitonin. • The thyroid hormones are synthesized and stored in the thyroid follicles as part of thyroglobulin molecule - which is a glycoprotein synthesized by thyroid cells. • Iodine is an element that plays an essential role in the functioning of a healthy thyroid. It is used for the production of thyroid hormones. • The total body content of I2, obtained from food and water, is 30 - 50 mg. Ref: https://www.btf-thyroid.org/iodine-and-thyroid
- 9. Thyroid Hormones - Actions • The actions of T4 and T3 are qualitatively similar and are nicely depicted in the features of hypo- and hyperthyroidism. • Increases the basal metabolic rate. • Depending on the metabolic status, it can induce lipolysis or lipid synthesis. • Stimulate the metabolism of carbohydrates. • Anabolism of proteins. Thyroid hormones can also induce catabolism of proteins in high doses. • Permissive effect on catecholamines. • In children, thyroid hormones act synergistically with growth hormone to stimulate bone growth. The impact of thyroid hormone in CNS is important. During the prenatal period, it is needed for the maturation of the brain. • In adults, it can affect mood. Hyperthyroidism can lead to hyperexcitability and irritability. Hypothyroidism can cause impaired memory, slowed speech, and sleepiness. • Thyroid hormone affects fertility, ovulation, and menstruation. Ref: https://www.ncbi.nlm.nih.gov/books/NBK500006/
- 10. Thyroid Hormones - Disorders • Hyperthyroidism • Hypothyroidism • Graves Disease • Hashimoto Thyroiditis Ref: https://www.ncbi.nlm.nih.gov/books/NBK500006/
- 11. Relation between T4 and T3 • Thyroid secretes more T4 than T3. • T4 is the major circulating hormone because it is 15 times more tightly bound to plasma proteins. • T3 is 5 times more potent than T4 and acts faster. Peak effect of T3 comes in 1–2 days while that of T4 takes 6– 8 days. • T3 is the active hormone, while T4 is mainly a transport form which functions as a prohormone of T3. Preparations • l-thyroxine sod. (synthetic levothyroxine sod.) • 25 - 150 μg tabs
- 12. Thyroid hormones preparation - uses • The most important use of thyroid hormone is for replacement therapy in deficiency states. • Cretinism: Due to failure of thyroid development or a defect in hormone synthesis or due to extreme iodine deficiency. • Adult hypothyroidism (Myxoedema): This is one of the commonest endocrine disorders which develops as a consequence of autoimmune thyroiditis or thyroidectomy. • Myxoedema coma: It is an emergency; characterized by progressive mental deterioration due to acute hypothyroidism carries significant mortality. • Nontoxic goiter: Enlargement of thyroid with euthyroid status. • Thyroid nodule: It is solid or fluid-filled lumps that form within thyroid. • Papillary carcinoma of thyroid
- 13. Thyroid inhibitors • These are drugs used to lower the functional capacity of the hyperactive thyroid gland. • Thyrotoxicosis is due to excessive secretion of thyroid hormones due to Graves’ disease and toxic nodular goiter.
- 14. Antithyroid drugs - Thioamides • Thioamides (propylthiouracil, methimazole and carbimazole) act principally by blocking the synthesis of T4 by preventing iodination of tyrosine residues. • Propylthiouracil also inhibits peripheral conversion of T4 to T3. • Carbimazole is rapidly converted to thiaimazole, the active metabolite. • Thioamides cross the placenta, propylthiouracil less than carbimazole. • Adverse effects: Hypothyroidism and goiter Ref: doi: 10.1016/B978-0-443-10281-3.00016-6
- 15. Inhibit iodide trapping • Inhibit iodide trapping by Sodium iodide symporter (NIS) into the thyroid. • Consequently, T4/T3 cannot be synthesized. Ref:
- 16. Inhibit hormone release IODINE, RADIOACTIVE IODINE • Iodine is a constituent of thyroid hormones; it is the fastest acting thyroid inhibitor. • Use: • Preoperative preparation: Thyroidectomy in Graves’ disease - Iodine is generally given for 10 days just preceding surgery. • Thyroid storm • Prophylaxis of endemic goiter • Antiseptic Ref:
- 17. Treatment • Treatment of hypothyroidism: • Levothyroxine • Treatment of hyperthyroidism (thyrotoxicosis): • Removal of the thyroid • Inhibition of thyroid hormone synthesis • Blockade of hormone release • Thyroid storm Ref:
- 18. Pancreatic Hormones Drug altering the pancreatic hormones secretion
- 20. Functions of pancreas Ref: https://biology.reachingfordreams.com/biology/endocrine-system/14-function-of-pancreas-in-human-body Pancreatic polypeptide cells (PP cells)
- 21. Functions of pancreas • The pancreas made up of two types of tissues that independently function as exocrine and endocrine glands. • Exocrine part of the pancreas secretes digestive enzymes into the duodenum. • Endocrine portion of the pancreas secretes glucagon and insulin, two non-steroid protein hormones. These hormones regulate the body’s metabolism of glucose and other carbohydrate molecules. They are produced by the islets of Langerhans. Ref: https://biology.reachingfordreams.com/biology/endocrine-system/14-function-of-pancreas-in-human-body
- 22. Exocrine Functions • Amylase: Secreted in mouth and pancreas; breaks down complex carbohydrates. • Lipase: Secreted in the pancreas; breaks down fats • Protease: Secreted in the pancreas; breaks down proteins. Endocrine Functions • Glucagon: Glucagon plays an important role in blood glucose regulation; low blood glucose levels stimulate its release. • Insulin: Elevated blood glucose levels stimulate the release of insulin. • Gastrin and amylin: Secreted in the pancreas; breaks down proteins
- 23. Islets of Langerhans • There are three main types of cells in the pancreatic islets: • α (alpha) cells produces the hormone glucagon [Glucagon increases blood glucose levels] • β (beta) cells produces the hormone insulin [insulin reduces blood glucose levels] • δ (delta) cells secrete somatostatin [inhibits the secretion of both insulin and glucagon]
- 24. Common pancreatic problems and digestion • Diabetes • Type I Insulin-dependent diabetes mellitus (IDDM)/ juvenile onset diabetes mellitus • Type II Noninsulin-dependent diabetes mellitus (NIDDM)/ maturity onset diabetes mellitus • Pancreatitis • Pancreatic cancer
- 25. Diabetes • The incidence of diabetes is growing rapidly worldwide. • Malaysia has the highest rate of diabetes in Western Pacific region and one of the highest in the world and costing around 600 million US dollars per year. • The prevalence of diabetes raised from 11.2% in 2011 to 18.3% in 2019, with a 68.3% increase. According to a national survey report, in Malaysia in 2019, 3.6 million adults had diabetes. Diabetes is expected to affect 7 million Malaysian adults aged 18 and older by 2025. Ref: PMID: 35085366
- 26. Comparison of type 1 and type 2 diabetes
- 27. Insulin • Insulin is a two-chain polypeptide having 51 amino acids and MW about 6000. The A-chain has 21 while B-chain has 30 amino acids. Under basal condition ~1U insulin is secreted per hour by human pancreas. Human proinsulin
- 28. Insulin • Mechanism of action: Exogenous insulin is administered to replace absent insulin secretion in type 1 diabetes or to supplement insufficient insulin secretion in type 2 diabetes. • Pharmacokinetics: Insulin is a polypeptide; it is degraded in the gastrointestinal tract if taken orally. Therefore, it is generally administered by subcutaneous injection. Inhaled insulin formulation is also available • Adverse effects: Hypoglycemia, weight gain, local injection site reactions, and lipodystrophy. Hypoglycaemia is managed by administering glucose (or glucose yielding carbohydrate, e.g., sugar) 15–20 g orally reverses the symptoms.
- 29. Insulin preparations • Rapid-acting and short-acting insulin preparations • Intermediate-acting insulin • Long-acting insulin preparations • Insulin combinations • Insulin delivery devices
- 30. Insulin preparations • Rapid-acting and short-acting insulin preparations: • Five preparations fall into this category: regular insulin, insulin lispro, insulin aspart, insulin glulisine, and inhaled insulin. • Regular insulin (peck level at 50 to 120 minutes) is a short-acting, soluble, crystalline zinc insulin. • Insulin lispro (peck level at 30 to 90 minutes), aspart, and glulisine are classified as rapid- acting insulins. • Inhaled insulin is also considered rapid-acting. This dry powder formulation is inhaled and absorbed through pulmonary tissue, with peak levels achieved within 45 to 60 minutes. • Regular insulin should be injected subcutaneously 30 minutes before a meal, whereas rapid-acting insulins are administered in the 15 minutes proceeding a meal or within 15 to 20 minutes after starting a meal. • Rapid-acting insulin suspensions are commonly used in external insulin pumps, and they are suitable for IV administration.
- 31. Insulin preparations • Intermediate-acting insulin: Neutral protamine hagedorn (NPH) insulin is an intermediate-acting insulin formed by the addition of zinc and protamine to regular insulin. NPH insulin is used for basal (fasting) control in type 1 or 2 diabetes and is usually given along with rapid- or short-acting insulin for mealtime control. NPH insulin should be given only subcutaneously (never IV). • Long-acting insulin preparations: It has a slower onset than NPH insulin and a flat, prolonged hypoglycemic effect with no peak. Eg: Insulin glargine, Insulin degludec.
- 32. Insulin preparations • Insulin combinations: Various premixed combinations of human insulins [70% NPH insulin + 30% regular insulin/ 50% NPH insulin + 50% regular insulin]. Use of premixed combinations decreases the number of daily injections but makes it more difficult to adjust individual components of the insulin regimen. • Insulin delivery devices: • Syringes • Pens • Durable pens • Pumps • Jet injectors • Others
- 33. Oral antidiabetic drugs • These drugs lower blood glucose levels in diabetics and are effective orally. The main drawback of insulin is - it must be given by injection.
- 35. Oral hypoglycemic agents, dose range and dose frequency MEDICINE USUAL DAILY DOSE FREQUENCY Glibenclamide 5 mg 2.5–20 mg • Up to 10 mg as a single dose • >10 mg in divided doses • Taken with or immediately before food Glipizide 5 mg 2.6–40 mg • Up to 15 mg as a single dose • >15 mg in a twice daily dosage taken • immediately before meals Gliclazide 80 mg 30–120 mg • Daily Glimepiride 1/ 2 mg 1–4 mg • 2–3 per day Metformin 500 mg, 1g 0.5–1.5 g • 1–3 times/day taken with or immediately after food Repaglinide 0.5 mg, 1/ 2 mg 0.5–16 mg • 2–3 per day Pioglitazone 15 mg, 30 mg 4–8 mg • Daily Rosiglitazone 2 mg, 4 mg 4–8 mg • Daily Acarbose 50/ 100 mg 50–100 mg • TDS with food thrice a day Voglibose 0.2/ 0.3 mg 0.2–0.3 mg • TDS with food thrice a day Sitagliptin 50/ 100 mg 100 mg per day in BD regimen. In combination with metformin, or a sulfonylurea • With or without food Vildagliptin 50 mg • With or without food
- 36. Corticosteroids Drug altering the Corticosteroids secretion
- 37. Corticosteroids • Corticosteroids are a class of steroid hormones released by the adrenal cortex, which includes glucocorticoids and mineralocorticoids. • Glucocorticoids are primary stress hormones that regulate a variety of physiologic processes and are essential for life. • Use: • Corticosteroids used to treat conditions like Asthma, Allergic rhinitis and hay fever, Urticaria, Atopic eczema, Chronic obstructive pulmonary disease (COPD), Painful and inflamed joints, Muscles and tendons, Lupus, Inflammatory bowel disease (IBD) including Crohn's disease and ulcerative colitis, Giant cell arteritis and polymyalgia rheumatica and, Multiple sclerosis (MS). Ref: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4662771/ https://www.nhsinform.scot/tests-and-treatments/medicines-and-medical-aids/types-of-medicine/corticosteroids
- 38. Corticosteroids
- 39. Corticosteroids
- 40. Uses: • Replacement therapy • Acute adrenal insufficiency • Chronic adrenal insufficiency (Addison’s disease) • Congenital adrenal hyperplasia (Adrenogenital syndrome) Ref:
- 41. Uses: • Pharmacotherapy (for nonendocrine diseases) • Arthritides (Rheumatoid arthritis, Osteoarthritis, Rheumatic fever, Gout) • Collagen diseases (systemic lupus erythematosus, polyarteritis nodosa, dermatomyositis, nephrotic syndrome, • Glomerulonephritis and related diseases) • Severe allergic reactions • Autoimmune diseases (Autoimmune haemolytic anaemia, idiopathic thrombocytopenic purpura, active chronic hepatitis) • Bronchial asthma and lung diseases • Infective diseases • Eye diseases • Skin diseases • Intestinal diseases • Neurological conditions Ref: • Nausea and vomiting • Malignancies • Organ transplantation • Septic shock • Thyroid storm
- 42. Adverse effects • Mineralocorticoid: Sodium and water retention, edema, hypokalaemic alkalosis and a progressive rise in BP. • Glucocorticoid: • Weight gain • Feeling very hungry • Water retention or swelling • Mood swings • Blurred vision • Feeling nervous or restless • Trouble sleeping • Muscle weakness • Acne • Stomach irritation, etc., Ref:
- 43. Androgens Drug altering the androgens secretion
- 44. Androgens and Related Drugs • Androgens (Male Sex Hormones) are substances which cause development of secondary sex characters in the castrated male. Testes of adult male produce 5–12 mg of testosterone daily. • Actions: • Testosterone is responsible for all the changes that occur in a boy at puberty • Testosterone accelerates erythropoiesis by increasing erythropoietin production and probably direct action on haeme synthesis. • Preparations and Dose: • Testosterone (free): 25 mg i.m. daily to twice weekly • testo. propionate 25 mg + testo. enanthate 100 mg in 1 ml amp; 1 ml i.m. weekly • Transdermal androgen Delivery of androgen
- 45. Androgens and Related Drugs Ref:
- 46. Estrogens, Progestins and Contraceptives
- 47. Estrogens • Estrogens (Female Sex Hormones) it helps develop and maintain both the reproductive system and female characteristics. • Actions: • The estrogens bring about pubertal changes in the female including growth of uterus, fallopian tubes and vagina. • Estrogens augment rhythmic contractions of the fallopian tubes and uterus. • Secondary sex characters. • Estrogen is important in maintaining bone mass primarily by retarding bone resorption. • Preparations and Dose: • Estradiol benzoate/cypionate/enanthate/valarate: 2.5–10 mg i.m • Conjugated estrogens: 0.625–1.25 mg/day oral • Use: • Hormone replacement therapy (HRT)
- 48. Estrogens Ref:
- 49. Progestins • Progestin (favouring pregnancy) plays an essential role in pregnancy and fertility. Progestin convert the estrogen primed proliferative endometrium to secretory and maintain pregnancy after conception. • Actions: • The main function of progesterone is preparation of the uterus for nidation and maintenance of pregnancy. • Preparations and Dose: • Progesterone: 10–100 mg i.m. OD • Hydroxyprogesterone caproate: 250–500 mg i.m. at 2–14 days intervals • Lynestrenol (Ethinylestrenol): 5–10 mg OD oral • Use: • Hormone replacement therapy (HRT), As contraceptive, Dysfunctional uterine bleeding, Endometriosis, Premenstrual syndrome/tension, Endometrial carcinoma
- 50. Progestins
- 51. Antiprogestin • Mifepristone: Given during the follicular phase, its antiprogestin action results in attenuation of the midcycle Gn surge from pituitary. This causes slowing of follicular development and delay/ failure of ovulation. • Uses: • Termination of pregnancy (of up to 7 weeks: 600 mg as single oral dose causes complete abortion in 60–85% cases). To improve the success rate, current recommendation is to follow it up 48 hours later by a single 400 mg oral dose of misoprostol (synthetic prostaglandin). • Ulipristal: Inhibits ovulation by suppressing LH surge as well as by direct effect on follicular rupture.
- 53. Oxytocin and Other Drugs Acting on Uterus
- 54. Oxytocin and Other Drugs Acting on Uterus Ref: • The two main physical functions of oxytocin are to stimulate uterine contractions in labor and childbirth and to stimulate contractions of breast tissue to aid in lactation after childbirth.
- 55. Thank you Ref: