the ladakh protest in leh ladakh 2024 sonam wangchuk.pptx
The issues with prosthetic biomaterials
1. 1
Artificial Tissue Engineering
Dr. Munira Shahbuddin
The issues with prosthetic biomaterials.
1. Relevance ofbioartificial materials in regenerative medicine.
In any organ or tissues, the ECM components provide the means by which adjacent cells
communicate with each other and the external environment for ECM organization, composition
impact of organ development and function.
The vital interface between ECM and cell components is mainly provided by transmembrane cell
surface receptors, integrins, which ensure communication and mediate bidirectional signalling across
the cell membrane. Binding of integrins to ECM results in the activation of cascade of events called
signalling that influences cellular morphology, proliferation, differentiation and survival.
Engineering biomimetic scaffold would enable the modulation of cellular response and regulation of
cell behaviour.
The use of natural and synthetic polymers should meet the requirement of the physiological
environment that match tissue regeneration process. This includes its mechanical properties,
reproducible chemistry and times of degradation. Cell affinity towards synthetic polymers is generally
poor as a consequence of their low hydrophilicity and lack of surface cell recognition sites.
The use of hydrolysed polymers such as PLA, PGA, PLGA and PCL that degrade into polymer of 10-
40 micron particles that are capable of being phagocytosed and metabolised to carbon dioxide and
water is in the favour due to its controlled degradation property.
Typical natural polymers like polysaccharides and proteins are very attractive as cells are components
of carbohydrate moieties of their membrane proteoglycans, GAG, glycoprotein while proteins, such as
collagen, fibronectin, fibrin, laminin etc are natural components of the ECM and display functional
motif peptides that specific for cell surface receptors.
The current approach of regenerative medicine is to design a custom based tissue specific biomaterials
by the incorporation of the key characteristics of naturally derived materials into purposely selected or
synthesized synthetic polymers.
2. Biocompatibility and Immune response to biomaterials.
The mechanisms of host innate and humoral response to whole organ transplantation are reasonably
well understood. Xenogenic and allogenic cellular antigens are recognised by the host, elicit immune
activation and cause the production of proinflammatory mediators with downstream cytotoxicity and
transplantation of organ/tissue rejection.
There are considerations that should be taken into note, time to transplantation, patient-donor human
leukocyte antigen (HLA) matching.
Tissue engineering and regenerative medicine strategies for organ transplantation offer the potential
of custom made organs composed of patient’s own cells, presumably avoiding complications off
allogenic antigens.
2. 2
Each strategy may differ in the specific combination of cells, biomaterials and bioactive factors
selected for the application.
3. Transplant rejection.
Rejection is driven via the recognition of nonself alloantigen (primarily MHC, major
histocompatibility complex class I) on cells of the donor organ and activation of the acquired immune
response (CD4+ and CD8+ T cells).
In the absence of immune suppression, this response occur within 10-13 days post-transplantation
(acute rejection).
Subsequent tissue or organ from the same donor will be subjected to a accelerated rejection response
within 6-8 days due to a memory-type immune response.
MHC or Human Leukocyte Antigen (HLA) is a potent driver of the acquired immune response to
transplanted organ.
Rejection can happen due to mismatch of genetic loci.
Antigen presenting cells (APC) bearing both alloantigen and costimulatory molecules activated T
cells by recognizing the pathways of direct or indirect allorecognition. The activation of rejection
response via the direct pathway can be reduced by depletion of donor APC within the organ prior to
transplantation or in cases of transplantation without lympathic drainage.
Antibodies also play an important role in the rejection response. Hyperacute rejection result from the
interaction of antibodies and the subsequent complement cascade with the vascular endothelium
leading to clotting and loss of blood supply to transplanted organ.
Hyperacute rejection can be avoided by screening of blood types and for the presence of reactive
alloantibodies prior to transplant.
For the same reason, xenografts are unsuitable for human transplant as for example α-Gal epitope on
the cells of other mammals is rapidly recognized by pre-existing antibodies in humans, leading to
acute rejection.
Alloreactivities by the recruitment of innate immune cells (monocytes and macrophages) by T cells
lead to chronic inflammation, scarring, and subsequent graft failing.
T cells activation involved in both acception and rejection of allo/xeno transplantation with activation
of Th1 and Th2 lymphocyte phenotypes.
Th1 lymphocytes produce cytokines such as interleukin 1 (IL-1), interferon γ (IF-γ) and tumor
necrosis factor - β (TNF-β) leading to macrophages activation, stimulation of complement fixing
antibody isotypes and differentiation of CD8+ cells to cytotoxic type.
Th2 lymphocytes produce IL-4, IL-5, IL-6 and IL-10, cytokines that do not activate macrophages and
that lead to the production of noncomplement fixing antibodies.
The phenotype of the activated T cekks is the critical difference and the paradigm of Th1/Th2 will be
further discussed in the host response to tissue injury. Nonetheless, it is important to appreciate the
transplant rejection response as aspects of the acquired immune system that may be activated
3. 3
depending on the type of cells used and their source also its dependent upon the noncellular
components used to construct the organ.
4. The host response to tissue injury.
The response to trauma is a protective mechanism to prevent further insult to the host by hemorrage,
potential pathogens, loss of function or by a prolonged inflammatory response: commonly known as
wound healing.
The host response to tissue injury is generally considered to occur in four overlapping stages,
eventually leading to the deposition of scar tissue consisting of dense fibrous connective tissue.
5. Wound healing response
Hemostasis - Inflammation - Proliferative Phase - Remodelling Phase
5.1 Mechanism ofwound healing
Wound healing is a complex, physiological self repairing process in which injured skin (or other
organ tissues) undergoes progressions of physiological events to restore its functional normality
(Joseph 2004). Human skin has one of the greatest ability to regenerate itself compared to other
tissues in our body. The normal healing process starts as soon as the tissue is injured where the blood
components come into contact with collagen and ECM at the site of injury, releasing clotting and
growth factors (Joseph 2004). This progression is divided into three sequential and overlapping
phases; inflammatory, proliferative and remodeling at which can be characterized by secretion of
distinctive cytokines by specific cells.
5.1.1Inflammation
Inflammatory phase plays important roles in fighting infections, clearance of debridement and
induction of proliferative phase (Joseph 2004). During the time of injury, hemostasis or clotting
cascade takes place in order by a way of a fibrin clot. Stimultaneously, the cells launch chemokines
and cytokines to attract cells to phagocytose debris, bacteria and damaged tissue that give
recognizable cardinal sign of inflammatory response such as redness, warmth, swelling, pain and loss
of function. Inflammatory phase can be divided into four subphases: coagulation, vasoconstriction and
vasodilation, polymorphonuclear neutrophils and macrophages (Braun and Werner 2006).
i. Coagulation
Coagulation is part of hemostasis and it started as soon as injury took place, triggering
inflammatory factors by initiating extrinsic coagulation cascade to activate factor VII. Factor VII is an
essential blood clotting factor for hemostasis. Exposure of tissue factors such as thrombokinase with
blood leads to a formation of fibrin plug by mediating crosslinking of fibrin and fibronectin. Fibrin
plug act as a structural support to prevent blood loss and also as a matrix for migratory cells. It allows
platelet to adhere and express glycoproteins on their cell membranes. Glycoproteins allow them to
stick to each other and aggregate (Joseph 2004). Platelet secrete adenosine diphosphate, tissue growth
factor-β (TGF-β) and platelet derived growth factor (PDGF) to act on surrounding cells and stimulate
chemotaxis of neutrophil, monocytes and fibroblasts to the wound site, thus promoting the increase of
cell proliferation and migration (Joseph 2004).
4. 4
ii. Vasoconstriction and vasodilation
Vasoconstriction of constriction of blood vessel happens immediately after a blood vessel is breached,
causing the ruptured cell membranes to release inflammatory factors such as thromboxane and
prostaglandin. This is to prevent blood loss and a mechanism to aid the injured site by collecting
inflammatory cells and factors. Vasoconstriction lasts five to ten minutes and is followed by a
widening of blood vessels. This peaks at about twenty minutes post-wounding (Joseph 2004).
Histamine is the main cause of vasodilation as it causes the blood vessels to become porous and
facilitates the entry of the inflammatory cells like leukocytes from the blood stream into the wound
site (Joseph 2004).
iii. Polymorphonuclear Neutrophils (PMNs)
PMNs arrive at the wound site within hours of injury and begin to dominate the cells in the wound for
the first fourty eight hours of injury together with white blood cells (WBC). They are the first to begin
bactericidal activity using inflammatory mediators and oxygen free radicals in what is called a
‘respiratory burst’. Normal wound healing can occur without PMNs and it normally undergo apatosis
after completion of their tasks which later be engulfed and degraded by macrophages (Joseph 2004).
iv. Macrophages
Unlike PMNs, macrophages are essential to wound healing as it involve in debridement, fibroblasts
proliferation and angiogenesis. After 24-36 hours as PMNs begin to decrease, circulating monocytes
will enter the wound and mature into tissue macrophages. These macrophages are important to
debridement of damaged tissue in microscopic level by phagocytozing bacterias and debris. Also, in
the process of debridement, they produce a wide range of important substances such as interleukin-1
(IL-1) and basic fibroblast growth factor (bFGF) (Metcalfe and Ferguson 2007).
At this stage, IL-1 and bFGF is important to the proliferation of inflammatory cells and promotion of
angiogenesis through endothelial cells replication. Towards the end of the inflammatory phase,
creation of granulation tissues (eicosanoids) in the wound will strongly influence fibroblasts
proliferation and synthesis of collagen as well as promoting the influx of keratinocytes and
endothelial to the wound (Li, Zhang et al. 2003; Yamaguchi, Hearing et al. 2005).
5.1.2 Proliferative Phase
The proliferative phase is characterized by angiogenesis, collagen deposition, granulation tissue
formation, reepithelization and wound contraction. It begins when mononuclear cells continuously
replacing white blood cells (WBC) and macrophages. At two to three days after injury, fibroblasts
from the wound margin will migrate inward over the fibrous matrix which formed during the
inflammatory phase. At the same time, formation of new blood vessels (angiogenesis) by endothelial
cells is taking place and the step is overlap with other proliferative stages such as fibroplasia over time
(Joseph 2004).
i. Angiogenesis (Neovascularization)
Angiogenesis or neovascularization is a regeneration of new blood vessel. The process is normal and
vital in wound healing and concurrenly happening with fibroblasts proliferation and endothelial cells
migration. Cooperative regulation of vascular endothelial growth factor (VEGF), angiopoietic,
fibroblast growth factor (FGF) and transforming growth factor-β (TGF-β) are essentials as they
5. 5
fascilitate endothelial expansion to angiogenesis, creating vessels in granulation tissues. This process
is directly stimulated by hypoxia condition which is a low oxygen environment and the presence of
lactic acid. Production of angiogenic factors by macrophages and the other growth factors producing
cells will stop when they are no longer in a hypoxic and lactic acid filled environment, leading to
reduction of endothelial migration and proliferation (Li, Zhang et al. 2003). At the end of this stage
when tissue is perfuse with adequate nutrients and environment, the blood vessels that are no longer
needed will die by apoptosis (Li, Zhang et al. 2003).
ii. Fibroplasia and granulation tissue formation
Fibroplasia and granulation tissue formation begin as the inflammatory phase ends and
simultaneously starting with angiogenesis. At this stage fibroblasts is beginning to accumulate in the
wound and soon will become the dominant type peaking at one to two weeks. Fibroblasts use fibrin
linked fibers to migrate across the wound and then begin to assemble collagen molecules into the
fibers (Joseph 2004).
Fibroblast is also one of the important components in granulation tissues that appear rudimentarily
since the inflammatory phase. As angiogenesis stopped, granulation tissues containing newly formed
blood vessels, endothelial cells, myofibroblasts and components of a new provisional extracellular
matrix (ECM) will grow continuously until the wound bed is covered (Gouin and Kiecolt-Glaser ;
Joseph 2004; Metcalfe and Ferguson 2007).
Provisional ECM is different with ECM found in non-injured tissue and this will later be replaced by
fibroblast in the next phase of healing (Joseph 2004).
ii.i Collagen deposition
Fibroblast is the major contributor for collagen synthesis and deposition of collagen in fibril linked
fibers increase the strength of the wound, facilitating cells that involve in angiogenesis, inflammation
and construction of connective tissues to adhere,grow and differentiate.
The type III collagen and fibronectin are begin to be produced at approximately ten hours to three
days after injury and their deposition peak length from one to three weeks depending on the size of
the wound (Joseph 2004).
iii. Epithelization
Reepithelization takes place from the formation of granulation tissues in an open wound that allows
epithelial cells and keratinocytes to migrate across the newly formed tissue to form a barrier between
the wound and the surrounding (Braun and Werner 2006). In this stage, keratinocytes do not undergo
proliferation yet but its migration from wound edges across the wounded site is important to allow
formation of epithelial cells that would later assist in further healing stage.
Before migration, keratinocytes will change its shape into longer and flatter morphologies thus
extending their cellular processes such as further formation of actin filament and lamellipodia. The
migration is mediated by the lack of contact inhibition and chemicals such as nitric oxide (Schwentker,
Vodovotz et al. 2002). They use fibronectin linked fibrin that was formed during inflammatory phase
to move across the wound site. During this stage, epithelial cells are forming at wound edges to
provide a base for keratinocytes proliferation. The epithelial cells are also important to remove debris
(debridement) and contagions.
6. 6
Keratinocytes migration will continue until cells from other wound edges meet to form a contact
inhibition which causes them to stop migrating. As this happen, they will secrete proteins that form
the new basement membrane and established desmosomes and hemidesmosomes to anchor the layer
to the basement membrane (Eves, Beck et al. 2005).
iii.i Contraction
Wound contracture is a normal physiological event in wound healing defined as ‘the dimunition of
area of a wound that occurs from centripetal movement of the whole thickness of the surrounding
tissue (Abercrombie, Flint et al. 1956; Yannas 2005). Contraction is vital for wound healing and it
commences approximately 4 to 5 days after wounding at an everage of 0.6-0.7 mm.day-1 depending
on tissue type and wound shape (Lawrence 1998). The contraction appeared to be mediated by
fibroblastic lineage when fibroblasts differentiated into myofibroblasts (Eichler and Carlson 2006) but
the exact nature of myofibroblasts interaction with ECM has yet to be determined (Tejero-Trujeque
2001). The process begins 4 to 5 days after wounding and continues for 12-15 days depending on
tissue type and wound shape (Lawrence 1998). It also can lasts up to several weeks depending on the
severity of the wound and prolonged contration can cause severe limitation of functions and skin
deformation.
5.1.3 Maturation and Remodelling
Remodelling begins when collagen deposition is adequate for reepithelization to mature and
production of collagen type III is gradually replaced by collagen type I (Isaac, Mathor et al. 2009).
The tensile of the wound will increase over time and will become as much as 80% as strong as normal
tissue at least 12 weeks after injury.
6. Foreign body reaction
Foreign body reaction is well accepted for biomaterials, particularly for nondegradable synthetic and
metallic components intended for long term implantation. The host response include:
6.1 Blood material interaction with the
deposition of a protein film on a biomaterial
6.2 Provisional matrix formation
6.3 Acute inflammation
6.4 Chronic inflammation
6.5 Granulation tissue formation
6.6 Foreign body reaction
6.7 Fibrosis and capsule development.
6.1 Blood material interaction
Release of blood into the wound site results in degranulation of platelets, formation of a provisional
matrix as was described in wound healing.
The proteins that absorb to a biomaterial may include components of the coagulation system
(fibrinogen and tissue factor), complement cascade (C5) and other plasma derived proteins (albumin
and IgG).
These proteins provide a substrate with which the inflammatory cells arriving at the site of injury
interact at the surface of biomaterials. Interactions of cells with protein absorbed at the biomaterials
7. 7
may lead to variety of a cellular responses including adherence, or triggering phagocytic pathways, all
depending on the cell type and proteins involved.
6.2 Acute inflammation.
This happened at the emigration of neutrophils from the vasculature into the implant site, follows the
formation of the provisional matrix and the release of chemoattractant factors by platelets and other
cells within the inflammatory site.
Adsorption of fibronectin and IgG plays significant roles in the Mac-1 mediated attachment of
neutrophils and macrophages to biomaterial surfaces during the acute phase of inflammation.
Complement and serum immunoglobulin adsorption to a pathogen (term opsonisation) leads to
phagocytosis by neutrophils and/or macrophages or destruction of the pathogen via the complement
pathway.
Opsonized biomaterials elicit phagocytosis or will be subjected to frustrated phagocytosis, leading to
the release of microbicidal content at the surface of foreign body. This may lead to the erosion of a
biomaterial, and eventually lead to a failure of the material to perform as intended.
6.3 Chronic inflammation.
This associated with the implantation of a biomaterial, which characterized by the presence of
activated macrophages. The process of macrophages accumulation may occur for a period of days to
months, depending on the nature of biomaterials.
The continued presence of macrophages at the site of biomaterial implantation is often the precursor
to the formation of granulation tissue, the foreign body giant cell response and the eventual
encapsulation of the biomaterial within a dense layer of collageneous connective tissue.
6.4 Granulation tissue formation, foreign body reaction and tissue encapsulation.
Chronic inflammation can progress to a granulation tissue phase in which the deposition of new ECM
and the robust angiogenesis into the implantation site are conspicuous.
The persistence of granulation tissue combined with the presence of a non degradable biomaterial is
eventually associated with the formation of foreign body giant cells. Factors such as protein
adsorption to the biomaterial, that interact with cell surface integrin receptors regulate macrophage
behaviour.
In the final stage of the host response following implantation of a biomaterial is an increasingly dense
layer of collagenous connective tissue is deposited around the surface of the material, thus isolating or
encapsulating it from the surrounding healthy tissue.
6.4 Macrophage polarization.
In the host response to pathogen and cancer immunology, macrophages have been shown to have
heterogenous phenotypes ranging from M1 (classically activated, proinflammatoy) to M2 (anti-
inflammatory, homeostatic, wound healing), mimicking the Th1/Th2 pathways.
8. 8
M1 are activated by well known proinflammatory signals such as IL-1β, IL-6, IL-12, IL23 and TNFα,
produce high levels of reactive oxygen species (ROS) and efficient APC, the cause of inducer and
effector cells in Th1 pathway.
M2 are activated by molecular cues such as IL-4, IL-13, IL-10 and immune complexes, the high level
of IL-10 have increased the expression of scavenger, mannose and galactose receptors, produce
ornithine and polyamines in place of ROS and involved in the polarized Th2 type reaction.
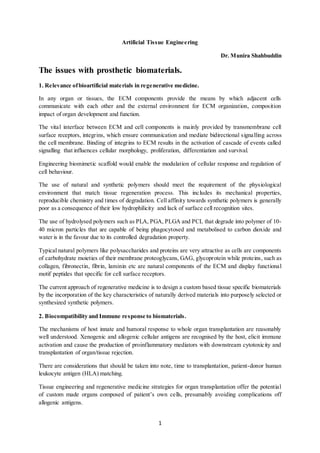
Figure. Macrophage polarization paradigm.
A) common inducers, surface molecule expression, cytokines and effector molecule production,
nuclear translocation and functional characteristics of recognized macrophage subsets as described by
Mantovani et. al. Macrophage polarization occurs on a spectrum between M1 and M2 extremes.
Macrophage phenotype is plastic and can change with paracrine and autocrine signals. Therefore there
is logical that macrophages may adopt a transitional phenotype and functions as both M1 and M2.
Triangles represent secreted reactive species and circles replresent secreted cytokines.
Arg- arginase, C/EPBβ, CCAAT/- enhancer binding protein beta, CCR,C-C - chemokine receptor, CD - cluster of
differentiation, IC - immune complex, LPS – lipopolysaccharide, IFN-γ – interferon γ, IL – interleukin, iNOS – inducible
nitric oxide synthase, RNI – reactive nitrogen intermediates, TLR – toll like receptor, TNFα – tumor necrosis factor α, STAT
– signal transducer and activator of transcription, ROI – reactive oxygen intermediates.
Conclusion Increased understanding of the necessary and determinant role of macrophages in tissue
remodelling following injury, a number of studies have begun to apply similar paradigms to the
outcomes observed in tissue engineering and regenerative medicine approaches to tissue
9. 9
reconstruction. It has been observed that strategies which promote transition from M1 to more
friendly M2 are better able to promote constructive tissue remodelling and recovery of function than
those which promote only M1 response or lead to a foreign body reaction.