VIROLOGY - RABIES VIRUS
•
6 likes•1,764 views

Morphology, Pathogenesis, Labdiagnosis and Treatment of Rabies Virus

Recommended
More Related Content
What's hot
What's hot (20)
Similar to VIROLOGY - RABIES VIRUS
Similar to VIROLOGY - RABIES VIRUS (20)
More from Meenatchisundaram Subramani
More from Meenatchisundaram Subramani (12)
Recently uploaded
Recently uploaded (20)
VIROLOGY - RABIES VIRUS
- 1. Dr. S. MEENATCHISUNDARAM ASSOCIATE PROFESSOR DEPARTMENT OF MICROBIOLOGY SNMV COLLEGE OF ARTS AND SCIENCE COIMBATORE https://orcid.org/0000-0002-8691-449X 95496 https://scholar.google.com/citations?user=IkdZ5XsAAAAJ&hl=en RABIES VIRUS
- 2. INTRODUCTION Rabies is an acute infection of the central nervous system that is almost always fatal. The virus is usually transmitted to humans from the bite of a rabid animal. Although the number of human cases is small, rabies is a major public health problem because it is widespread among animal reservoirs. The viruses are classified in the family Rhabdoviridae. Rabies viruses belong to the genus Lyssavirus The rhabdoviruses are very widely distributed in nature, infecting vertebrates, invertebrates, and plants. Rabies is the only medically important rhabdovirus. Many of the animal rhabdoviruses infect insects, but rabies virus does not.
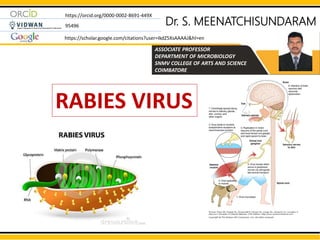
- 3. MORPHOLOGY Rhabdoviruses are rod- or bullet-shaped particles measuring 75 x 180 nm. The particles are surrounded by a membranous envelope with protruding spikes, 10 nm long. The peplomers (spikes) are composed of trimers of the viral glycoprotein (G). Inside the envelope is a ribonucleocapsid. The genome is single-stranded, negative-sense RNA (12 kb; MW 4.6 x 106). Virions contain an RNA-dependent RNA polymerase.
- 4. MORPHOLOGY Genome The core of the virion consists of helically arranged ribonucleoprotein. The genome is single-stranded RNA, linear, nonsegmented, negative-sense. RNA-dependent RNA polymerase enzyme which is essential for the initiation of replication of the virus, is enclosed within the virion in association with the ribonucleoprotein core. Proteins Protruding from the lipid envelope are approximately 200 glycoprotein (G) spikes of the virus, hemagglutinin activity. Spikes do not cover the planar end of the virion. Membrane or matrix (M) protein Beneath the envelope is the membrane or matrix (M) protein and is the major structural protein of the virus which may be invaginated at the planar end
- 5. RESISTANCE Rabies virus survives storage at 4 °C for weeks and at -70 °C for years. It is inactivated by CO2, so on dry ice it must be stored in glass-sealed vials. Rabies virus is killed rapidly by exposure to ultraviolet radiation or sunlight, by heat (1 hour at 50 °C), by lipid solvents (ether, 0.1% sodium deoxycholate), by trypsin, by detergents, and by extremes of pH.
- 6. STREET VIRUS - FIXED VIRUS STREET VIRUS The rabies virus isolated from natural human or animal infection is termed the street virus. Following inoculation by any route, it can cause fatal encephalitis in laboratory animals after a long and variable incubation period of about 1–12 weeks (usually 21–60 days in dogs). Intracytoplasmic inclusion bodies (Negri bodies) can be demonstrated in the brain of animals dying of street virus infection. FIXED VIRUS After several serial intracerebral passages in rabbits, the virus undergoes certain changes and becomes what is called the fixed virus that no longer multiplies in extraneural tissues. The fixed (or murant) virus is more neurotropic, though it is much less infective by other routes. After intracerebral inoculation, it produces fatal encephalitis after a short and fixed incubation period of 6–7 days. Negri bodies are usually not demonstrable in the brain of animals dying of fixed virus infection. The fixed virus is used for vaccine production.
- 7. ANTIGENIC PROPERTIES Glycoprotein G: The surface spikes are composed of glycoprotein G, which is important in pathogenesis, virulence and immunity. Purified spikes containing the viral glycoprotein elicit neutralizing antibody in animals. The purified glycoprotein may therefore provide a safe and effective subunit vaccine. Hemagglutinating activity: Rabies virus possesses hemagglutinating activity, optimally seen with goose erythrocytes at 0–4 °C and pH 6.2. Hemagglutination is a property of the glycoprotein spikes. The hemagglutinin antigen is species specific and distinct from the antigens on rabies related viruses.
- 8. ANTIGENIC PROPERTIES Nucleocapsid protein Complement fixing antibodies are induced by the nucleocapsid protein and are not protective. This antigen is group specific and cross-reactions are seen with some rabies related viruses. Antiserum prepared against the purified nucleocapsid is used in diagnostic immunofluorescence for rabies. Other antigens Other antigens identified include two membrane proteins, glycolipid and RNA dependent RNA polymerase.
- 9. PATHOGENESIS Rabies virus multiplies in muscle or connective tissue at the site of inoculation Then enters peripheral nerves at neuromuscular junctions and spreads up the nerves to the central nervous system. However, it is also possible for rabies virus to enter the nervous system directly without local replication. It multiplies in the central nervous system and progressive encephalitis develops. The virus then spreads through peripheral nerves to the salivary glands and other tissues. The organ with the highest titers of virus is the submaxillary salivary gland. Other organs where rabies virus has been found include pancreas, kidney, heart, retina, and cornea. Rabies virus has not been isolated from the blood of infected persons.
- 10. PATHOGENESIS Rabies infection usually results from the bite of rabid dogs or other animals. The virus present in the saliva of the animal is deposited in the wound. The virus appears to multiply in the muscles, connective tissue or nerves at the site of deposition. The virus remains at the site for days to months before progressing to the central nervous system (CNS). Rabies virus travels by retrograde axoplasmic transport to the dorsal root ganglia and to the spinal cord. Once the virus gains access to the spinal cord, the brain becomes rapidly infected. The virus then disseminates from the CNS via afferent neurons to highly innervated sites, such as the skin of the head and neck, salivary glands, retina, cornea, nasal mucosa etc. The virus ultimately reaches virtually every tissue in the body, though the centrifugal dissemination may be interrupted at any stage by death. Rabies is fatal once clinical disease is apparent.
- 11. PATHOGENESIS
- 12. PATHOGENESIS Susceptibility to infection and the incubation period may depend upon Host's age Genetic background Immune status Viral strain involved Amount of inoculum The severity of lacerations The distance the virus has to travel from its point of entry to the central nervous system. There is a higher attack rate and shorter incubation period in persons bitten on the face or head; the lowest mortality occurs in those bitten on the legs.
- 13. CLINICAL FINDINGS Rabies is primarily a disease of lower animals and is spread to humans by bites of rabid animals or by contact with saliva from rabid animals. The incubation period in humans is typically 1–2 months but may be as short as 1 week or as long as many years (up to 19 years). It is usually shorter in children than in adults. The clinical spectrum can be divided into three phases: a short prodromal phase, an acute neurologic phase and coma. The prodrome, lasting 2–10 days, may show any of the following nonspecific symptoms: malaise ( general feeling of discomfort) Anorexia (anorexia, is an eating disorder) Headache, photophobia Nausea and vomiting Sore throat Fever Usually there is an abnormal sensation around the wound site.
- 14. CLINICAL FINDINGS During the acute neurologic phase, which lasts 2–7 days, patients show signs of nervous system dysfunction such as Nervousness Apprehension (a fear that something unpleasant is going to happen) Hallucinations (A hallucination is the experience of seeing something that is not really there because you are ill or have taken a drug.) Bizarre (very strange or unusual) behavior. General sympathetic overactivity is observed, including Lacrimation (the secretion of tears especially when abnormal or excessive) increased salivation and perspiration (the process of sweating) A large fraction of patients will exhibit hydrophobia (fear of water) The act of swallowing precipitates a painful spasm of the throat muscles. This phase is followed by seizures (A seizure is a sudden, uncontrolled electrical disturbance in the brain) or coma and death. The major cause of death is respiratory paralysis. Paralytic rabies occurs in about 20% of patients, most frequently in those infected with bat rabies virus. Recovery and survival are extremely rare.
- 15. LABORATORY DIAGNOSIS 1. Diagnosis of Human Rabies Tests are performed on samples of saliva, serum, spinal fluid, and skin biopsies of hair follicles at the nape of the neck. A. Rabies Antigens by Immunofluorescence The method most commonly used for diagnosis is the demonstration of rabies virus antigens by immunofluorescence. The specimens tested are corneal smears and skin biopsy (from face or neck) or saliva and brain. Direct immunofluorescence is done using antirabies serum tagged with fluorescein isothiocyanate. The use of monoclonal antibody instead of crude antiserum makes the test more specific. B. Virus Isolation a. Mouse Inoculation Samples of brain tissue, saliva, CSF, or urine may be injected intracerebrally into newborn mice for isolation of the virus. Infection in mice results in encephalitis and death. The inoculated mice are examined for signs of illness and their brains are examined at death or at 28 days postinoculation for Negri bodies, or by immunofluorescence rabies antigen.
- 17. LABORATORY DIAGNOSIS b. Isolation in Cell Culture A more rapid and sensitive method is isolation of the virus in tissue culture cell lines (WI38, BHK21,CER). Virus isolations is identified by immunofluorescence. A positive IF test can be obtained as early as 2–4 days after inoculation. The identity of the isolate can be established by the neutralization test with specific antirabies antibody C. Serology Rabies antibodies can be detected in the serum and CSF of the patient by ELISA. High titer antibodies are present in the CSF in rabies but not after immunization. D. Detection of Nucleic Acid Reverse transcription-polymerase chain reaction (RT-PCR) testing can be used to amplify parts of a rabies virus genome from fixed or unfixed brain tissue for detection of rabies virus RNA. This technique can confirm dFA results and can detect rabies virus in saliva and skin biopsy samples.
- 18. PROPHYLAXIS A. Postexposure Prophylaxis B. Preexposure Prophylaxis A. Post-exposure Prophylaxis This consists of: a. Local treatment , b. Antirabic vaccines, c. Hyperimmune serum. a. Local treatment of wound: Cleansing: Immediate flushing and washing the wound(s), scratches and the adjoining areas with plenty of soap and water, preferably under a running tap, for at least 5 minutes as soap inactivates virus by destroying its envelope. Chemical treatment: After cleansing wound should be inactivated by irrigation with virucidal agents - either alcohol (400–700 ml/liter), tincture or 0.01% aqueous solution of iodine or povidone iodine. Suturing: Bite wounds should not be immediately sutured. Antirabies Serum: The local application of antirabies serum or its infiltration around the wound has been shown to be highly effective in preventing rabies. Antirabic vaccines: Antirabic vaccines fall into two main categories: neural and non-neural The former are associated with serious risk of neurological complications and have been replaced by the latter.
- 19. TYPES OF ANTIRABIC VACCINES I. Neural vaccines Pasteur's Cord Vaccine Fermi vaccine Semple vaccine Beta-propiolactone (BPL) vaccine Suckling mouse brain vaccine II. Non-neural vaccines a. Egg vaccines Duck egg vaccine (DEV) Live attenuated chick embryo vaccine b. Tissue culture vaccine Human diploid cell vaccine (HDCV) Purified chick embryo cell culture vaccine (PCECV) Rabies vaccine Adsorbed (RAV) Purified Vero cell rabies vaccine (PVRV) BHK - Rabies Vaccine c. Subunit vaccine
- 20. ANTIRABIC VACCINES – NEURAL VACCINES I. Neural Vaccines These are suspensions of nervous tissues of animals infected with the fixed rabies virus. Pasteur's Cord Vaccine: Prepared by Louis Pasteur in 1885 by drying pieces of infected rabbit spinal cord over caustic potash for varying periods. Fermi Vaccine: Preparations of infected brain treated with phenol Semple Vaccine: 5% suspension of sheep brain infected with fixed virus and inactivated with phenol at 37°C Beta propiolactone (BPL) vaccine: Similar to semple vaccine, but the inactivating agent is beta propiolactone and supposed to be more antigenic Infant mouse brain vaccine: Vaccine prepared from suckling mouse brain (scanty or absence of myelin in nerve tissue) and inactivated by UV irradiation, beta propiolactone or phenol
- 21. II. Non-neural Vaccines 1. Egg vaccine Duck embryo vaccine (DEV): The rabies virus is grown in embryonated duck eggs. Anaphylactic reactions are infrequent but the antigenicity of the vaccine is low, so that many (16–25) doses have to be given to obtain a satisfactory postexposure antibody response. It is no longer manufactured. Live attenuated chick embryo vaccines These vaccines were used for vaccination of animals. Two types of vaccines were developed with the Flury strain. i. Low Egg Passage (LEP) vaccine: at 40–50 egg passage level for immunization of dogs. ii. High Egg Passage (HEP) vaccine: at 180 passage level for cattle and cats. These are not in use now. ANTIRABIC VACCINES – EGG VACCINE
- 22. ANTIRABIC VACCINES - TISSUE CULTURE VACCINE 2. TISSUE CULTURE VACCINE Human Diploid Cell Vaccine (HDCV): Vaccine developed in 1964 by growing fixed virus (Wistar’s Pitman-Moore strain) on human diploid cell (WI-38 or MRC-5) and inactivated with beta propiolactone. Purified Chick Embryo Cell Culture Vaccine (PCECV): Flury LEP strain grown on chick embryo cell culture and inactivated by beta propiolactone. Rabies Vaccine, Adsorbed (RVA): The vaccine is prepared from the Kissling strain of rabies virus adapted to a diploid cell line of the fetal rhesus lung. The virus is inactivated with beta-propiolactone and concentrated by adsorption to aluminum phosphate. Vero Cell Vaccine (VRV): Viruses are grown in vero cells and inactivated by formaldehyde. The inactivated vaccine obtained from Vero cells, required a purification step in order to remove the residual cellular DNA, hence is known as the purified Vero cell rabies vaccines (PVRV). BHK-Rabies Vaccine: Rabies virus strain L. Pasteur (Vero cell adapted) grown on BHK-21 C13 cell monolayers, inactivated with beta-propiolactone and adsorbed on Aluminum phosphate. (Still in trial stage)
- 23. ANTIRABIC VACCINES – RECOMBINANT VACCINES Subunit Vaccine The glycoprotein subunit on the virus surface, which is the protective antigen, has been cloned and recombinant vaccines produced. They are still in the experimental stage. Passive Immunization Passive immunization is an important adjunct to vaccination and should be invariably employed whenever the exposure is considered of high risk. Two preparations of anti rabies serum are available for passive immunization Horse Antirabies Serum: It should be given on day 0 in a single dose of 40 IU/kg of body weight subject to a maximum of 3000 Units. Human Rabies Immune Globulin: Human rabies immune globulin (HRlG) has now replaced equine antirabies serum in many countries. The dose recommended is a single administration of 20 IU per kg of body weight. ANTI RABIES SERUM
- 24. POSTEXPOSURE PROPHYLAXIS Postexposure Prophylaxis The decision to administer rabies antibody, rabies vaccine-or both- depends on several factors: (1) The nature of the biting animal and its vaccination status (2) The availability of the animal for laboratory examination (3) The existence of rabies in the area (4) The manner of attack (5) The severity of the bite and contamination by saliva of the animal (6) Advice from local public health officials. Postexposure prophylaxis requires five or six doses, on days 0, 3, 7, 14, 30 and optionally 90. The vaccineis to be given intra muscular (1M) or subcutaneous (SC) in the deltoid region, or in children on the anterolateral aspect of the thigh.
- 25. B. Preexposure Prophylaxis This is indicated for persons at high risk of contact with rabies virus such as laboratory workers handling rabies virus or with rabid animals (veterinarians). Preexposure prophylaxis requires three doses of the vaccine injected on day 0, 7, 21 or 0, 28 and 56. A booster dose is recommended after one year and then one every five years. PREEXPOSURE PROPHYLAXIS
- 26. TREATMENT There is no successful treatment for clinical rabies. Interferons, ribavirin, and other drugs have shown no beneficial effects. Symptomatic treatment may prolong life, but the outcome is almost always fatal. Preexposure vaccination is desirable for all persons who are at high risk of contact with rabid animals, such as veterinarians, animal care personnel, certain laboratory workers, and spelunkers. Persons traveling to developing countries where rabies control programs for domestic animals are not optimal should be offered preexposure prophylaxis if they plan to stay for more than 30 days. However, preexposure prophylaxis does not eliminate the need for prompt postexposure prophylaxis if an exposure to rabies occurs.
Editor's Notes
- This template was inserted from Power-user, the productivity add-in for PowerPoint and Excel. Get thousands of templates, icons, maps, diagrams and charts with Power-user. Visit www.powerusersoftwares.com!