
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Rabies virus
Similar to Rabies virus (20)
More from Crimson College of Technology (Pokhara University)
More from Crimson College of Technology (Pokhara University) (14)
Recently uploaded
Recently uploaded (20)
Rabies virus
- 2. INTRODUCTION:- Rabies has been known since around 2000 BC. The first written record of rabies is in the Mesopotamian Codex of Eshnunna (circa 1930 BC), which dictates that the owner of a dog showing symptoms of rabies should take preventive measure against bites. If another person were bitten by a rabid dog and later died, the owner was heavily fined.
- 4. Structure of Rabies Virus The virus is enveloped, rod shaped particles measuring 75 × 180 nm. Mature virion appears either as bullet shaped particles with one rounded and one flattened end or as bacilliform particles. The particles are surrounded by a membranous lipid envelope. The particles have a buoyant density in CsCl of about 1.19 g/cm3. The virion outer surface is covered with protruding spikes which is 10nm long. The peplomers (spikes) are composed of trimers of the viral glycoprotein. Inside the envelope is a ribonucleocapsid which encloses single-stranded, negative- sense RNA genome (12 kb; molecular weight 4.6 *10ˆ6). The genome encode for five proteins designated as glycoprotein(G), nucleoprotein(N), phosphoprotein(P), matrix protein(M) and large polymerase protein(L).
- 6. Genome of Rabies Virus The rabies virus genome is composed of approximately 12000 nucleotides. It is single-stranded RNA, linear, non-segmented, negative sense. The genomic RNA encodes for the five different viral proteins: nucleoprotein(N), phosphoprotein (P), matrix protein (M), glycoprotein (G) and the large polymerase protein (L). The viral ribonucleoprotein (RNP) core consists of the viral RNA encapsidated by N proteins and associated with the P and L proteins. The other viral proteins, M and G are involved in virion structure and attachment to cellular receptors, respectively. The intergenic region (G-L) is approximately 450 nucleotides in length and does not appear to encode any polypeptides.
- 7. Epidemiology of Rabies Virus Rabies infection in man is generally acquired from the bite of an infected animal. The domestic dog (Canis familiaris) is the most important vector, although bat rabies continues to cause human infection across much of Central and South America. The virus still remains endemic across much of the developing world, where the majority (99%) of human deaths due to rabies occur, mainly in Africa and Asia although extensive vaccination campaigns in dog and terrestrial wildlife populations have reduced the incidence across globe. The World Health Organization (WHO) estimates an annual toll of 55 000 deaths following human infection with rabies virus, although this is likely to be a gross underestimate.
- 8. Transmission of Rabies Virus Bite of infected rabid animal Contact of saliva with broken skin or with mucous membrane Corneal transplant
- 9. Replication of Rabies Virus
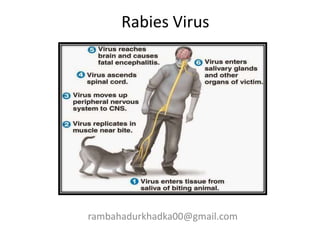
- 10. Pathogenesis of Rabies Virus
- 11. 1. After inoculation of infectious saliva by bite, virus may persist and replicate in muscle tissue before progressing to the peripheral nervous tissue via neuromuscular junction. 2. Neurotropsim is a main feature associated with viral replication residing exclusively to neurons. 3. A significant interaction of G protein and acetylcholine receptor provide evidence of viral attachment. 4. After peripheral nerve entry, virus moves centripetally within axons to the CNS via transportation by retrograde axonal flow 5. Incubation period is dependent on the distance between site of bite and CNS. 6. Apart from this, it also depends on age of host, immune status of host, viral strain involved and amount of inoculation. 7. In the CNS, the multiplication of the virus occurs in the grey matter and spreads in the endoneurium of Schwann cell. 8. Virus spread may be facilitated by movement across cell to cell junctions. 9. After period of multiplication, it disseminate into tissues and organs via efferent neurons.
- 12. Clinical manifestations of Rabies Virus The disease is an acute, fulminant, fatal encephalitis. The incubation period in humans is typically 1–3 months but may be as short as 1 week or more than a year. The clinical spectrum can be divided into three phases: a short prodromal phase, an acute neurologic phase, and coma.
- 13. The prodrome, lasting 2–10 days, may show any of the following nonspecific symptoms: malaise, anorexia, headache, photophobia, nausea and vomiting, sore throat, and fever. During the acute neurologic phase, which lasts 2–7 days, patients show signs of nervous system dysfunction such as nervousness, apprehension, hallucinations, and bizarre behavior. Beside these, general sympathetic overactivity is observed, including lacrimation, pupillary dilatation, and increased salivation and perspiration. Hydrophobia (fear of water) or aerophobia (fear when feeling a breeze) is exhibited by number of patients. The act of swallowing precipitates a painful spasm of the throat muscles. Neurologic phase is followed by convulsive seizures or coma and death. The major cause of death is cardiorespiratory arrest. The disease course is slower, with some patients surviving 30 days. However, recovery and survival are extremely rare.
- 14. Diagnosis of Rabies Virus Specimen: saliva, corneal biopsy, brain tissue, neck skin biopsy Histopathology Detection of Negri bodies by Seller’s staining technique which comprises use of basic fuchsin and methylene blue. Negri bodies are purplish pink, sharply demarcated, more or less spherical, and 2–10 μm in diameter, and they have a distinctive internal structure with basophilic granules in an eosinophilic matrix.
- 15. Antigen detection Tissues infected with rabies virus are currently identified most rapidly and accurately by means of immunofluorescence or immunoperoxidase staining using antirabies monoclonal antibodies. Antibody detection Antibodies develop slowly in infected persons or animals during progression of the disease but promptly after vaccination with cell-derived vaccines. Serum antibodies to rabies can be detected by immunofluorescence or neutralization tests.
- 16. Virus isolation Available tissue is inoculated intracerebrally into suckling mice. Infection in mice results in encephalitis and death. The central nervous system of the inoculated animal is examined for Negri bodies and rabies antigen. However, virus isolation takes too long to be useful in making a decision about whether to give vaccine. Molecular method Reverse transcription-polymerase chain reaction testing can be used to amplify parts of a rabies virus genome from fixed or unfixed brain tissue or saliva. Sequencing of amplified products using Nucleic Acid Sequence Based Amplification can allow identification of the infecting virus strain.
- 17. Treatment of Rabies Virus No successful treatment in clinical use
- 18. Management, Prevention and Control of Rabies Virus Avoid contact with wild and domestic animals Do not approach animals or attempt to pick up an unusually tame animal or one that appears unwell Do not attract stray animals by offering food or by being careless with litter Be aware that certain activities can attract dogs (e.g. running, cycling) Be aware that children are at higher risk of rabies as they are less likely to avoid contact with animals or report a lick or bite. Active immunization with modern tissue culture vaccines consists of a series of four doses, all administered intramuscularly in the deltoid region, 1 mL each, over a 2-week period (days 0, 3, 7, and 14). For persons with immunosuppression, the recommended postexposure prophylaxis series includes five doses of vaccine administered on days 0, 3, 7, 14, and 30. Use of both active and passive immunization is strongly recommended for proper treatment.
- 21. THANK YOU