Tetralogy of Fallot.pdf
•
0 likes•84 views

Tetralogy of Fallot Tetralogy of Fallot with Pulmonary Stenosis TETRALOGY OF FALLOT WITH CONGENITAL PULMONARY ATRESIA Tetralogy of Fallot with Absent Pulmonary Valve

Recommended
More Related Content
Similar to Tetralogy of Fallot.pdf
Similar to Tetralogy of Fallot.pdf (20)
More from KararSurgery
More from KararSurgery (12)
Recently uploaded
Recently uploaded (20)
Tetralogy of Fallot.pdf
- 2. Directed by DR.Karar .A.Ali department of cardiothoracic surgery kararbenign@gmail.com
- 3. •
- 4. •
- 5. •
- 6. •
- 7. •
- 8. •
- 9. •
- 10. •
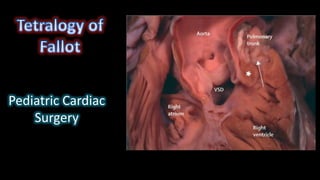
- 11. • An autopsied specimen has been opened through the anterior wall of the right ventricle to show the cardinal features of tetralogy of Fallot.
- 12. • In this specimen, opened in the same fashion as the heart shown in Figure 1, there is fibrous continuity between the leaflets of the aortic and tricuspid valves in the postero-inferior margin of the ventricular septal defect, making the defect itself perimembranous
- 13. • In this specimen, also photographed in a fashion comparable for the heart shown in Figure 1, there is muscular tissue interposed between the leaflets of the aortic and tricuspid valves in the postero-inferior margin of the ventricular septal defect.
- 14. • n this specimen, again photographed as for Figure 1, the defect extends to the level of the pulmonary valve due to failure of muscularisation of the outlet septum during development of the heart. This type of defect is doubly committed and juxtaarterial, but is also perimembranous.
- 15. • This specimen has tetralogy of Fallot with pulmonary atresia. The pulmonary supply is through multiple systemic-to-pulmonary collateral arteries. The star shows the connection between one of the collateral arteries and the intrapericardial pulmonary arteries. All the other arteries join with the intrapericardial pulmonary arterial supply, or else supply segments of the lung directly. The task of the clinician is to display the supply of the various collateral arteries and their communications with the intrapericardial pulmonary arteries.
- 16. • This still frame image of a parasternal short axis view of the echocardiogram of a patient with tetralogy of Fallot demonstrates the antero-cephalad deviation of the outlet septum into the right ventricular outflow tract.
- 17. •
- 18. • A slightly modified view (a), angled to optimize imaging of the pulmonary arteries in the patient imaged to produce Figure 6, reveals significant hypoplasia of the pulmonary trunk and the pulmonary arteries, which result from the antero- cephalad deviation of the outlet septum. The pulmonary valvar leaflets are not visualized. In panel b, colour Doppler has been used, and demonstrates turbulence and acceleration of the flow of blood in the right ventricular outflow tract, originating at the level of the deviated outlet septum. The turbulence continues into the hypoplastic pulmonary trunk and pulmonary arteries.
- 19. • “tetralogie” to refer to the aggregate of four features of the anatomy seen in the majority of specimens coming into his autopsy service from patients with “la maladie bleue”: pulmonary artery stenosis, ventricular septal communication, rightward deviation of the aorta’s origin, and hypertrophy of the right ventricle
- 20. • Tetralogy of Fallot Prevalence Tetralogy of Fallot occurs in 5% to 10% of all CHDs. This is probably the most common cyanotic heart defect
- 21. • Pathology 1. The original description of TOF included the following four abnormalities: a large VSD, RVOT obstruction, RVH, and overriding of the aorta. In actuality, only two abnormalities are required, a VSD large enough to equalize pressures in both ventricles and an RVOT obstruction. The RVH is secondary to the RVOT obstruction, and the overriding of the aorta varies
- 23. • 2. The VSD in TOF is a large perimembranous defect with extension into the subpulmonary region
- 24. • 3. The RVOT obstruction is most frequently in the form of infundibular stenosis (45%).The obstruction is rarely at the pulmonary valve level (10%). A combination of the two may also occur (30%). The pulmonary valve is atretic in the most severe form of the anomaly (15%), • 4. The pulmonary annulus and main PA are variably hypoplastic in most patients. The PA branches are usually small, although marked hypoplasia is uncommon. Stenosis at the origin of the branch PAs, especially the left PA, is common. Occasionally, systemic collateral arteries feed into the lungs, especially in severe cases of TOF
- 25. • 5. Right aortic arch is present in 25% of cases, with some of them having symptoms of vascular ring. 6. In about 5% of TOF patients, abnormal coronary arteries are present. The most common abnormality is the anterior descending branch arising from the right coronary artery and passing over the RVOT, which prohibits a surgical incision in the region. 7. Complete AV canal defect occurs in approximately 2% of patients with TOF, more commonly among patients with Down syndrome, called “canal tet.” In these patients, the VSD has a large outlet component in addition to the inlet portion associated with the AV canal
- 26. •
- 27. • What are the symptoms of a vascular ring? • stridor (noisy breathing) • wheezing or cough. • respiratory distress. • difficulty feeding when you introduce solid foods. • swallowing difficulties (dysphagia) • gastroesophageal reflux (GERD) • respiratory infections.
- 28. • Highlights • •The prevalence of coronary anomalies in TOF is 4– 6%. • •In patients with an ACA, 72% of the anomalous arteries cross the RVOT. • •The risk of encountering an ACA or large conus artery crossing the RVOT is 10.3%. • •Before surgery, define the coronary anatomy to avoid damage of anomalous vessel. • •Surgical approach should be adapted to the course of an anomalous coronary artery.
- 29. •
- 30. •
- 31. Figure 1: Pathology specimen showing a large coronary crossing the right ventricular outflow tract (black arrow). AA: Ascending aorta, LAA: Left atrial appendage, LCCA: Left common carotid artery, LV: Left ventricle, PT: Pulmonary trunk, RAA: Right atrial appendage, RCCA: Right common carotid artery, RV: Right ventricle, T: Thymus
- 32. •
- 33. • Figure 4: Origin of the LAD from the RCA crossing the right ventricular outflow tract. (a) High parasternal short-axis view. The enlarged proximal RCA supplies the LAD. (b) Leftward angled parasternal long-axis view profiling the right ventricular outflow tract (infundibulum) free wall. The LAD is seen in cross- section approximately 7 mm below the pulmonary valve[25] and 52-year-old male, status post TOF repair. (c) Anomalous origin of the LAD from the right coronary cusp (arrowhead). (d) The anomalous LAD courses anterior to the RVOT (arrows). (reproduced with permission from Kapur S, Aeron G, Vojta CN. Pictorial review of coronary anomalies in Tetralogy of Fallot. J Cardiovasc Comput Tomogr. 2015 Nov-Dec; 9(6):593-6.). A: Anterior, AoV: Aortic valve, Inf: Infundibulum, L: Left, LAD: Left anterior descending coronary artery, MPA: Main pulmonary artery, RCA: Right coronary artery, R/S: Right/superior, RVOT: Right ventricular outflow tract
- 34. • igure 5: Modification in the direction of right ventriculotomy when (a) left anterior descending coronary artery arises from right coronary artery (b) right coronary artery arises from left anterior descending coronary artery
- 35. • Figure 6: Van Son technique two parallel longitudinal incisions in main pulmonary artery are connected distally, thus creating a wide flap of pulmonary artery tissue. (a) The pulmonary artery flap is sutured to the superior edge of ventriculotomy (b) Oval-shaped glutaraldehyde-treated pericardial patch (or, alternatively pulmonary homograft patch) is circumferentially sutured to edges of ventriculotomy, pulmonary artery flap, and pulmonary arteriotomy
- 36. •Clinical Manifestations History 1. A heart murmur is audible at birth. 2. Most patients are symptomatic with cyanosis at birth or shortly thereafter. Dyspnea on exertion, squatting, or hypoxic spells develop later even in mildly cyanotic infants 3. Occasional infants with acyanotic TOF may be asymptomatic or may show signs of CHF from a large left-to-right ventricular shunt.
- 37. • Physical Examination • 1. Varying degrees of cyanosis, tachypnea, and clubbing (in older infants and children) are present. • 2. An RV tap along the left sternal border and a systolic thrill at the upper and mid-left sternal borders are commonly present (50%). • 3. An ejection click that originates in the aorta may be audible. The S2 is usually single because the pulmonary component is too soft to be heard. A long, loud (grade 3 to 5 of 6) ejection-type systolic murmur is heard at the mid-and upper left sternal borders. This murmur originates from the PS but may be easily confused with the holosystolic regurgitant murmur of a VSD. The more severe the obstruction of the RVOT, the shorter and softer the systolic murmur. • 4. In the acyanotic form, a long systolic murmur, resulting from VSD and infundibular stenosis, is audible along the entire left sternal border, and cyanosis is absent. Thus, auscultatory findings resemble those of a small-shunt VSD (but, unlike VSD, the ECG shows RVH or BVH).
- 38. • An ECG may be helpful in the diagnosis of tetralogy of Fallot. Findings on an ECG suggestive of tetralogy of Fallot include right axis deviation, right ventricular hypertrophy, wide QRS, and right bundle branch block
- 39. • Electrocardiography 1. Right-axis deviation (RAD) (+120 to +150 degrees) is present in cyanotic TOF. In the acyanotic form, the QRS axis is normal. 2. RVH is usually present, but the strain pattern is unusual (because RV pressure is not suprasystemic). BVH may be seen in the acyanotic form. RAH is occasionally present.
- 40. • Radiography Cyanotic Tetralogy of Fallot 1. The heart size is normal or smaller than normal, and pulmonary vascular markings are decreased. “Black” lung fields are seen in TOF with pulmonary atresia. 2. A concave main PA segment with an upturned apex (i.e., “boot- shaped” heart or coeuren sabot) is characteristic (Fig. 14-19). 3. RA enlargement (25%) and right aortic arch (25%) may be present. Acyanotic Tetralogy of Fallot Radiographic findings of acyanotic TOF are indistinguishable from those of a small to moderate VSD (but patients with TOF have RVH rather than LVH on the ECG).
- 41. •
- 42. • Tetralogy of Fallot and tracheoesophageal fistula Neonate with "boot-shaped" heart consistent with subsequently proven tetralogy of Fallot. Nasogastric tube is coiled in proximal esophagus, transparency of esophagus is interrupted on lateral view, and distal esophagus apparently connected to trachea by continuous lucency that represents tracheoesophageal fistula.
- 43. • Patient has history of corrective surgery for Tetralogy of Fallot. There is a stent in the RVOT conduit. Subtracted energy view. Bone energy view.
- 44. •
- 45. •
- 46. •
- 47. • VSD
- 49. • Echocardiography Two-dimensional echocardiography and Doppler studies usually make the diagnosis and quantitate the severity of TOF. 1. A large, perimembranous infundibular VSD and overriding of the aorta are readily imaged in the parasternal long-axis view (Fig. 14-20). • 2. Anatomy of the RVOT, the pulmonary valve, the pulmonary annulus, and the main PA and its branches is imaged in the parasternal short-axis and subcostal short-axis views. These views allow systematic evaluation of the severity of obstruction at different levels. • 3. Doppler studies estimate the pressure gradient across the RVOT obstruction.
- 50. • 4. Anomalous coronary artery distribution can be imaged accurately by echocardiographic studies (Fig. 14-21). The major concern is to rule out any branch of the coronary artery crossing the RVOT. Thus, preoperative cardiac catheterization solely for the diagnosis of coronary artery anatomy is not necessary. 5. Associated anomalies such as ASD and persistence of the left superior vena cava (LSVC) can be imaged.
- 51. •
- 52. •
- 53. • Natural History 1. Infants with acyanotic TOF gradually become cyanotic. Patients who are already cyanotic become more cyanotic as the infundibular stenosis worsens and polycythemia develops. 2. Polycythemia develops secondary to cyanosis.* 3. Physicians need to watch for the development of relative iron-deficiency states (i.e.,hypochromia) 4. Hypoxic spells may develop in infants 5. Growth retardation may be present if cyanosis is severe.* 6. Brain abscess and cerebrovascular accident rarely occur 7. Subacute bacterial endocarditis (SBE) is occasionally a complication.* 8. Some patients, particularly those with severe TOF, develop aortic regurgitation (AR). 9. Coagulopathy is a late complication of a long-standing cyanosis.*
- 54. • Hypoxic Spell Hypoxic spells (also called cyanotic spells, hypercyanotic spells, “tet” spells) of TOF are not as common as they used to be because many of the patients with TOF receive surgery before they develop the spells. However, it is very important for physicians to be able to immediately recognize and treat the spells appropriately because they can lead to serious complications of the CNS. Hypoxic spells are characterized by a paroxysm of hyperpnea (i.e., rapid and deep respiration), irritability and prolonged crying, increasing cyanosis, and decreasing intensity of the heart murmur. Hypoxic spells occur in infants, with a peak incidence between 2 and 4 months of age. These spells usually occur in the morning after crying, feeding, or defecation. A severe spell may lead to limpness, convulsion, cerebrovascular accident, or evendeath. There appears to be no relationship between the degree of cyanosis at rest and the likelihood of having hypoxic spells
- 55. • Treatment of the hypoxic spell strives to break the vicious circle of the spell. Physicians may use one or more of the following to treat the spell. 1. The infant should be picked up and held in a knee–chest position. 2. Morphine sulfate, 0.2 mg/kg administered subcutaneously or intramuscularly, suppresses the respiratory center and abolishes hyperpnea (and thus breaks the vicious cycle). 3. Oxygen is usually administered, but it has little demonstrable effect on arterial oxygen saturation. 4. Acidosis should be treated with sodium bicarbonate (NaHCO3), 1 mEq/kg administered IV. The same dose can be repeated in 10 to 15 minutes. NaHCO3 reduces the respiratory center– stimulating effect of acidosis.
- 56. • With the preceding treatment, the infant usually becomes less cyanotic, and the heart murmur becomes louder, which indicates an increased amount of blood flowing through the stenotic RVOT. If the hypoxic spells do not fully respond to these measures, the following medications can be tried: 1. Ketamine, 1 to 3 mg/kg (average, 2 mg/kg) administered IV over 60 seconds, works well. It increases the systemic vascular resistance (SVR) and sedates the infant. 2. Propranolol, 0.01 to 0.25 mg/kg (average, 0.05 mg/kg) administered by slow IV push, reduces the heart rate and may reverse the spell.
- 57. • Management Medical 1. Physicians should recognize and treat hypoxic spells It is important to educate parents to recognize the spells and know what to do. • 2. Oral propranolol therapy, 0.5 to 1.5 mg/kg every 6 hours, is occasionally used to prevent hypoxic spells while waiting for an optimal time for corrective surgery in the regions where open heart surgical procedures are not well established for small infants. • 3. Balloon dilatation of the RVOT and pulmonary valve, although not widely practiced, has been attempted to delay repair for several months. • 4. Relative iron-deficiency states should be detected and treated. Iron-deficient children are more susceptible to cerebrovascular complications. Normal hemoglobin or hematocrit values or decreased red blood cell indices indicate an iron-deficiency state in cyanotic patients
- 58. • Balloon Dilation of the Pulmonary Valve in Premature Infants with TOF
- 59. • Palliative Shunt Procedures Indications. Shunt procedures are performed to increase PBF (Fig. 14-22). Indications for shunt procedures vary from institution to institution. Many institutions, however, prefer primary repair without a shunt operation regardless of the patient’s age. However, when the following situations are present, a shunt operation may be chosen rather than primary repair. 1. Neonates with TOF and pulmonary atresia 2. Infants with hypoplastic pulmonary annulus, which requires a transannular patch for complete repair 3. Children with hypoplastic PAs 4. Unfavorable coronary artery anatomy 5. Infants younger than 3 to 4 months old who have medically unmanageable hypoxic spells 6. Infants weighing less than 2.5 kg
- 60. •
- 61. •
- 62. •
- 63. • Background • The original approach to performing a modified Blalock-Taussig (MBT) shunt is via a left thoracotomy. However, the median sternotomy has become the preferred approach of many surgeons. We think that the upper ministernotomy approach provides several advantages and avoids the disadvantages of both the sternotomy and thoracotomy approaches. Here, we describe our experience in constructing neonatal MBT shunts via upper ministernotomy.
- 64. • Results • Mean age was 16.9 ± 10.4 days, and weight was 3.5 ± 0.5 kg. All patients received grafts of size 3.5 mm. The mean oxygen saturation increased from 59.5 ± 7.3% preoperatively to 84.8 ± 4.2% postoperatively. There were three cases of mortality (6%). One patient suffered from an unstable sternum (2%). No patients required conversion to full sternotomy. Superficial wound infection occurred in three cases (6%), and there were no cases of mediastinitis. Mean duration of ventilation was 55.64 ± 37.5 h, mean ICU stay was 5.44 ± 3.9 days, and mean hospital stay was 14.7 ± 7.2 days.
- 65. • Conclusion • Upper ministernotomy is a safe approach with good early results. It provides adequate exposure with limited surgical trauma. Emergency conversion to full sternotomy and initiation of cardiopulmonary bypass can be achieved easily. It avoids lung compression and respiratory compromise. Additional costs for specific instruments are not necessary.
- 66. •
- 67. •
- 68. •
- 69. • Operative procedure • All patients received intramuscular ketamine (3 mg/kg) for sedation and stress-free separation from their parents. In the operating room, patients were monitored using five-lead ECG, pulse oximetry (SpO2), capnography for end-tidal carbon dioxide (Drager PM 8040-CATO, lübeck, Germany), planter surface temperature, and invasive blood pressure. Central venous catheters and arterial catheters were inserted after induction of general anaesthesia. Mechanical ventilation was provided by a Narkomed anaesthesia machine (North American Drager, Telford, PA) with fractional inspiratory oxygen concentration (fiO2) maintained 0.9 and 1.0. The end- tidal carbon dioxide (CO2) was maintained between 35 and 40 mmHg, using a tidal volume of 10 mL/kg and respiratory rate adjusted according to age. Positive end-expiratory pressure of 2–5 cmH2o and inspiratory to expiratory ratio (I:E ratio) of 1:1.5–1:2 were used.
- 70. • All MBT shunt procedures were performed via upper ministernotomy. A small skin incision was made from 0.5 cm below the suprasternal notch to 1 cm below the sternal angle. Then, the manubrium and the sternum were divided longitudinally in a J-shaped manner, using Mayo scissors up to the level of the third right intercostal space. After opening the sternum, the right lobe of the thymus was excised; the innominate artery was dissected up to its branches, with dissection of the right subclavian artery. The pericardium was opened above the aorta and stay sutures were inserted. The right pulmonary artery, between the ascending aorta and the superior vena cava up to the upper lobar branch, was dissected.
- 71. • The systemic site of the shunt insertion was either the innominate or right subclavian artery, and the site of the distal anastomosis was the right pulmonary artery as close to the middle line as possible. • The systemic artery was partially clamped with a Cooley clamp, and a longitudinal arteriotomy was performed at the undersurface of the artery. A transversely cut polytetrafluoroethylene (Gore-Tex) tube graft (W. L. Gore & Associates, Inc., USA) was sutured end-to-side to the arteriotomy. The clamp was then released in situ to ensure good shunt flow and a competent anastomosis. The systemic artery was clamped again, and the shunt was flushed by heparinised saline to flush any thrombi, then the shunt was trimmed to the appropriate length. The right pulmonary artery was partially clamped with a Cooley clamp, and an end-to-side distal anastomosis was performed in the same way All neonates in this series received 3.5-mm grafts, and the ductus was not ligated. • Before closure, haemostasis was secured, and a retrosternal drain was inserted
- 72. •
- 73. • Postoperative events Postoperatively, all neonates were ventilated. After haemostasis was ascertained, heparin was administered as a continuous infusion at 10–20 units/kg/h and was later changed to an oral low dose of aspirin (5 mg/kg/day). All patients received a postoperative echocardiographic examination to check the patency of the shunt Mortality There were three in-hospital deaths (6%). The causes of death were low cardiac output, sepsis, and acute respiratory distress syndrome (ARDS).
- 74. •
- 75. • Figure 1: A right modified Blalock–Taussig shunt through right thoracotomy with shunt size of 4 mm after previous central shunt through median sternotomy.
- 76. •
- 77. • Procedures, Complications, and Mortality. Although several other procedures were performed in the past (see Fig. 14-22), a modified BT (Gore-Tex interposition) shunt is the only procedure performed at this time. 1. Classic BT shunt, anastomosed between the subclavian artery and the ipsilateral PA, is usually performed for infants older than 3 months because the shunt is often thrombosed in young infants. A right-sided shunt is performed in patients with left aortic arch; a left-sided shunt is performed for right aortic arch. 2. With a modified BT shunt, a Gore-Tex interposition shunt is placed between the subclavian artery and the ipsilateral PA. This is the most popular procedure for any age, especially for infants younger than 3 months of age. Whereas a left-sided shunt is preferred for patients with left aortic arch, a right-sided shunt is preferred for patients with a right aortic arch. The surgical mortality rate is 1% or less.
- 78. • 3. The Waterston shunt, anastomosed between the ascending aorta and the right PA, is no longer performed because of a high incidence of surgical complications. Complications resulting from this procedure included too large a shunt leading to CHF or pulmonary hypertension and narrowing and kinking of the right PA at the site of the anastomosis. This created difficult problems in closing the shunt and reconstructing the right PA at the time of corrective surgery. • 4. The Potts operation, anastomosed between the descending aorta and the left PA, is no longer performed either. It may result in heart failure or pulmonary hypertension, as in the Waterston operation. A separate incision (i.e., left thoracotomy) is required to close the shunt during corrective surgery, which is performed through a midsternal incision.
- 79. • Complete Repair Surgery. Timing of this operation varies from institution to institution, but early surgery is generally preferred. Indications and Timing 1. Oxygen saturation less than 75% to 80% is an indication of surgery by most centers. The occurrence of hypoxic spells is generally considered an indication for operation. 2. Symptomatic infants who have favorable anatomy of the RVOT and PAs may have primary repair at any time after 3 to 4 months of age, with some centers performing it even before 3 months of age. • Most centers prefer primary elective repair by 1 to 2 years of age even if they are asymptomatic, acyanotic (i.e., “pink tet”), or minimally cyanotic.
- 80. • Advantages cited for early primary repair include diminution of hypertrophy and fibrosis of the RV, normal growth of the PAs and alveolar units, and reduced incidence of postoperative ventricular arrhythmias, and sudden death. • 3. Mildly cyanotic infants who have had previous shunt surgery may have total repair 1 to 2 years after the shunt operation. • 4. Asymptomatic children with coronary artery anomalies may have the repair after 1 year of age, because a conduit placement may be required between the RV and the PA.
- 81. • Procedure. Total repair of the defect is carried out under cardiopulmonary bypass, circulatory arrest, and hypothermia. The procedure includes patch closure of the VSD,preferably through transatrial and transpulmonary artery approach (rather than right ventriculotomy, which is shown in Fig. 14-23); widening of the RVOT by division or resection of the infundibular tissue; and pulmonary valvotomy, avoiding placement of a fabric patch whenever possible (see Fig. 14-23). Widening of the RVOT without placement of patch is more likely to be accomplished if the repair is done in early infancy. However, if the pulmonary annulus and main PA are hypoplastic, transannular patch placement is unavoidable. Whereas some centers advocate placement of a monocusp valve at the time of initial repair, others advocate pulmonary valve replacement at a later time if indicated
- 82. •
- 83. •
- 84. • Mortality. For patients with uncomplicated TOF, the mortality rate is 2% to 3% during the first 2 years. Patients at risk are those younger than 3 months and older than 4 years, as well as those with severe hypoplasia of the pulmonary annulus and trunk. Other risk factors may include multiple VSDs, large aortopulmonary collateral arteries, and Down syndrome.
- 85. • Complications 1. Bleeding problems may occur during the postoperative period, especially in older polycythemic patients. 2. Pulmonary valve regurgitation may occur, but mild regurgitation is well tolerated. 3. Right bundle branch block (RBBB) on the ECG caused by right ventriculotomy, which occurs in more than 90% of patients, is well tolerated. 4. Complete heart block (i.e., <1%) and ventricular arrhythmia are both rare.
- 86. •
- 87. • Figures 1 and 2 Standard cardiopulmonary bypass with direct bicaval cannulation is achieved, even in the neonate, at a systemic temperature of 28°C to 32°C (cannulas removed for clarity). A vent is placed through the right superior pulmonary vein and cold blood cardioplegia administered after aortic cross clamping. A right atriotomy is made parallel and close to the right atrioventricular groove. Placing the incision in this location assists in the exposure by elevating the anterior wall of the right ventricle and tricuspid valve with the stay sutures inserted along the atriotomy. The ventricular septal defect is visible behind the anterior leaflet of the tricuspid valve. Traction sutures are placed in the anterior and septal leaflets of the tricuspid valve. In the neonate, a patent foramen ovale is generally left open, but is closed in older infants
- 88. •
- 89. • Figure 3 The traction sutures placed on the anterior and septal leaflets of the tricuspid valve are essential in providing exposure with minimal retractors in the field. Each suture is retracted directly toward the surgeon, which pulls the septum and VSD into view. A small right-angle retractor is then placed under the anterior leaflet and pulled superiorly. The anterior limb of the septal band is identified. A traction suture placed here can help in the visualization of the out flow tract and help in keeping the surgeon’s orientation. The traction suture placed in the anterior limb of the septal band, which marks the anterior edge of the VSD, can be very helpful in maintaining orientation and exposing the distal outflow tract. Anterior and superior to this point is the pathway to the pulmonary valve, and the marking suture serves as a useful frame of reference to avoid an incision into the VSD itself
- 90. •
- 91. • Figure 4 The malalignment VSD is exposed, but relief of the right ventricular outflow tract obstruction is performed first. In some cases, a small calibrated dilator can be passed retrograde through the pulmonary valve to assist in exposure. Although not generally necessary, this maneuver has been found to be helpful when first attempting transatrial repairs, particularly in very small patients
- 92. •
- 93. •
- 94. • Figure 5 (B) Gentle probing with the clamp is important to avoid creating injury to the septum. In neonates and infants, this is generally easy to do as there is little secondary hypertrophy and the muscle bundles appear as “discrete” bands, which can be encircled for division. Resection is unnecessary as the outflow tract will expand sufficiently. It is important to realize that, although uncommon, some patients will not be suitable for transatrial muscle division secondary to hypoplasia of the right ventricular outflow tract. In such cases, an outflow tract patch will be required to enlarge the area of hypoplasia
- 95. •
- 96. • Figure 6 (A and B) Following relief of right ventricular outflow obstruction, the VSD is closed. A continuous suture technique is preferred, beginning at the juncture between the anterior and posterior limbs of the septal band. The first arm of the suture is placed along the anterior limb and around the annulus of the aortic valve. The latter is exposed more easily after the muscle bundles are divided. This suture passes into the right atrium where the aortic and tricuspid valves come together at the ventriculoinfundibular fold
- 97. •
- 98. •
- 99. • Figure 6 (C-E) The opposite needle is then used to anchor the patch along the inferior limb of the septal band and along the septal leaflet of the tricuspid valve in the standard fashion using the usual techniques to avoid injury to the conduction system. It is often necessary to weave the suture under the chordal attachments of the tricuspid valve to avoid distortion. The two ends of the suture are tied over a small pericardial pledget. It is important to test the tricuspid valve with saline to ensure that the valve is fully competent. A suture placed at the anteroseptal commissure of the valve is occasionally needed to reinforce this area.
- 100. •
- 101. •
- 102. •
- 103. • Exposure of ventricular septal defect and right ventricular outflow tract through tricuspid valve. B: Infundibular resection is complete and pulmonic valve can be seen.
- 104. •
- 105. •
- 106. •
- 107. •
- 108. • Anomalous coronary artery. • Anomalous anterior descending coronary artery arising from the right coronary artery is considered a contraindication to a primary repair because it may require placement of a conduit between the RV and PA, which is usually performed after 1 year of age. However, it is often possible to enlarge the outflow tract through a transatrial approach and by placing a short outflow patch either above or below the anomalous coronary artery. Alternatively, when a small conduit is necessary between the RV and the PA, the native outflow tract should be made as large as possible through an atrial approach, so that a “double outlet” (the native outlet and the conduit) results from the RV
- 109. • Postoperative Follow-up 1. Long-term follow-up with office examinations every 6 to 12 months is recommended, especially for patients with residual VSD shunt, residual obstruction of the RVOT, residual PA obstruction, arrhythmias, or conduction disturbances. 2. Significant pulmonary regurgitation (PR) may develop after repair of TOF. Although the PR is well tolerated for a decade or two, moderate to severe PR may eventually develop with significant RV dilatation and dysfunction, requiring surgical insertion of a homograft pulmonary valve. Severe PR left untreated may result in irreversible anatomic and functional changes in the RV, but the ideal timing of the valve replacement has been controversial. RV function is best investigated by MRI; if MRI is contraindicated because of the presence of metallic objects or cardiac pacemaker, CT should be used.
- 110. • suggested criteria for surgical pulmonary valve replacement. a. Recommended criteria by Geva T (2006) is primarily based on RV regurgitant fraction: 1) RV regurgitation fraction ≥25% PLUS 2) Two or more of the following criteria a) RV end-diastolic volume index ≥160 mL/m2 (normal, <108 mL/m2) b) RV end-systolic volume index ≥70 mL/m2 (normal, <47 mL/m2) c) LV end-diastolic volume index ≥65 mL/m2 d) RV ejection fraction ≤45% e) RV outflow tract aneurysm
- 111. • f) Clinical criteria: exercise intolerance, syncope, presence of heart failure, sustained ventricular tachycardia, or QRS duration ≥180 msec (two last ones are known risk factors for sudden death)
- 112. •
- 113. • b. Recently, Lee C. et al (2012) have recommended the following cutoff values for optimal outcome. They found the systolic volume index to be more important than the diastolic volume index in determining the outcome of surgery. 1) RV end-systolic volume index ≥80 mL/m2 and 2) RV end-diastolic volume index ≥163 mL/m2
- 114. •
- 115. • 3. Some patients, particularly those who had Rastelli operation using valved conduit, develop valvular stenosis or regurgitation. Valvular stenosis may improve after balloon dilatation, but PR may worsen. A nonsurgical percutaneous pulmonary valve implantation technique developed by Bonhoeffer et al (2000) has been used successfully. It is marketed as the Melody transcatheter pulmonary valve (Medtronic, Minneapolis, MN) (see further discussion under TOF with pulmonary atresia in this chapter). • 4. Some children develop late arrhythmias, particularly ventricular tachycardia, which may result in sudden death. Arrhythmias are primarily related to persistent RVH as a result of unsatisfactory repair. • 5. Pacemaker therapy is indicated for surgically induced complete heart block or sinus node dysfunction. • 6. Varying levels of activity limitation may be necessary. • 7. For patients who have residual defects or have prosthetic material for repair, subacute bacterial endocarditis prophylaxis should be observed throughout life
- 116. •
- 117. •
- 118. •
- 119. •
- 120. •
- 121. •
- 122. •
- 123. •
- 124. •
- 125. •
- 126. •
- 127. •
- 128. •
- 129. •
- 130. •
- 131. • The delamination PV plasty
- 132. •
- 133. •
- 134. •
- 136. FIGURE 1. The drawing shows the various types of PV plasty procedures that can be performed in addition to PV balloon dilation: (A) dysplastic PV with commissure fusion (effective PV opening); (B) PV commissurotomy (true initial PV annulus diameter); (C) PV balloon dilation and (D) final PV annulus diameter; (E) simple additional PV plasty (including PV leaflet repair and resuspension); (F-G) complex additional PV plasty, including PV leaflet delamination (F) and patch augmentation when needed and resuspension (G).
- 137. FIGURE E1. A-D, An excised bovine heart model was used to better understand the delamination plasty technique that was used to extend the PV cusp coaptation area, especially in patients with a hypoplastic PV annulus. In this model, the normal PV was exposed and examined through a longitudinal incision in the pulmonary trunk. After excision of 1 cusp of the tricuspid PV (creating a gap in coaptation mimicking the gap after PV balloon dilation in patients with a very hypoplastic PV annulus), a delamination plasty was performed on the other 2 cusps, thus extending their coaptation surface. Both cusps were then extended with triangles of biological tissue substitute and resuspended from the sinotubular junction, resulting in complete coverage of the PV annular area, simulating a bicuspid PV. A, Normal tricuspid PV; (B) removal of 1 PV cusp; (C) PV cusp delamination and leaflet extension, and (D) functionally bicuspid PV.
- 138. •
- 139. Our previous results show that the PV annulus and function can be preserved in selected patients undergoing early surgical repair of TOF, by combining a transatrial- transpulmonary with a subpulmonary muscular resection, without interfering with the ventriculo-arterial junction. Our results allowed us to achieve significantly better PV competence and right ventricular function in the midterm, compared with classic TOF repair with the utilization of a transannular patch.11 In this study, we have shown that the vast majority of PVs in TOF are bicuspid or tricuspid (>90%), and this anatomy is the most favorable surgically for applying PV-preservation procedures, regardless of the degree of leaflet dysplasia. On the contrary, a unicuspid PV is almost impossible to enlarge adequately at the single commissure, particularly when it is associated with a very hypoplastic PV annulus
- 140. After our initial results,10,11 we expanded the applicability of this technique to patients with a smaller PV annulus (Z-score 3), by the addition of complex surgical plasty of the PV, in recent studies. The overall PV-preservation rate was 56% and ranged from 21% (during the initial 2 years of our experience) to 100% (dur- ing the last 2 years of our experience). The more-aggressive use of complex PV plasty techniques, which have been applied in a progressively increasing percentage of patients since 2011 (up to 80% during the past few years;
- 141. •
- 142. During the initial use of the delamination plasty proce- dure, we were concerned about the possibility of hematoma in the outflow myocardium or tearing or other failure of the delaminated valve leaflets. However, after a median time of 2 years, we have not seen any sign of PV dysfunction, right ventricular muscle hematoma, or other anomaly indicating failure of the PV plasty procedures. We believe that the low pressure in the pulmonary circuit is key to the success of this PV plasty technique, allowing us to be very aggressive in PV cusp extension.
- 143. In conclusion, the majority of patients with TOF have a bicuspid or tricuspid PV, which is the most favorable surgical anatomy for preserving the PV, independent of the presence or degree of leaflet dysplasia. We believe that the preservation of the PV annulus and PV function during early repair of TOF, by combining intraoperative PV balloon dilation and additional surgical procedures, can be extended to the majority of patients with classic TOF. The recent introduction of more-complex PV plasty techniques, including delamination plasty, allowed us to further extend the applicability of PV-preservation techniques.
- 144. •
- 147. • Effects of V-Plasty on the pulmonary valve function and RVOT Gradient
- 148. pulmonary valve leaflet augmentation for transannular repair of tetralogy of Fallot
- 149. •
- 150. •
- 151. • Results • Median age at repair was 8.9 months (interquartile range, 5.4-14.8). There was no operative mortality. Median follow-up was 6.25 years (interquartile range, 2.77-7.75). Freedom from severe pulmonary regurgitation (PR) was 85% (95% confidence interval [CI], 77%-90%) and 76% (95% CI, 66%-83%) at 1 and 5 years, respectively. Freedom from moderate or greater PR was 69% (95% CI, 60%-76%) and 30% (95% CI, 21%-39%) at 5 and 10 years, respectively. Three patients required pulmonary valve replacement for PR. Nine patients required pulmonary balloon valvuloplasty. Freedom from intervention for pulmonary valve stenosis was 98% (95% CI, 93%-99%) and 94% (95% CI, 87%-97%) at 1 and 5 years, respectively. One patient with severe PR had an indexed right ventricular volume >160 mL/m2. Use of expanded polytetrafluoroethylene resulted in a greater freedom from moderate or greater PR (log-rank test P < .001; Cox regression hazard ratio, 0.40; 95% CI, 0.25-0.63; P < .001).
- 152. • Conclusions • At midterm follow-up of transannular repair with pulmonary valve leaflet augmentation, severe PR occurs in less than 50% of patients. The expanded polytetrafluoroethylene patch performs better than pericardium.
- 153. • As a rule, any symptomatic TOF is repaired, provided the anatomy is clear. The role for palliative aorto-pulmonary shunts in TOF with pulmonary stenosis has become limited to a very small subset of patients, such as those with anomalous left anterior descending (LAD) artery crossing the RVOT, significant noncardiac problems, or contraindication to cardiopulmonary bypassas In our experience, shunts carrymuch morbidity as primary repair. Thus, symptomatic neonates with TOF usually undergo primary repair
- 154. • Standard cardiopulmonary bypass techniques with bicaval cannulation and mild hypothermia (32-341C) are usually employed. Intraoperative transesophageal echocardiogram is performed to assess the anatomy and adequacy of the repair. The surgical principles that allow us to have a high rate of pulmonary valve preservation are the following: The main pulmonary artery (MPA) is almost always opened and later patched, as it provides a better avenue to work on the pulmonary valve than the RVOT. A small incision (usually 1 cm) is liberally made right below the pulmonary annulus on the RVOT, with complete and meticulous eradication of subpulmonary and suprapulmonary stenoses. Some surgeons are reluctant to make an incision in the RVOT, preferring to divide obstructing muscle bundles though the tricuspid valve and the pulmonary valve. A detailed analysis of the pulmonary valve anatomy and sinuses, noting the number of cusps, the number of commissures, and planes of the cusp, in particular the anterior cusp, is done. This inspection is more important than the preoperatively measured z score that only informs on the pulmonary annular size and not on valve morphology, repairability, or effective orifice.
- 155. • Based on this information, a decision is made whether to (1) just perform pulmonary valve thinning and commissur-otomy, • (2) add intraoperative balloon dilation, or • (3) perform a patch augmentation of the pulmonary valve. A classic transannular patch has now become a rare event.
- 156. • A patent foramen ovale (PFO) (2-3 mm) is almost always left behind as decompressing outlet for early RV dysfunction. • Mortality for standard TOF surgery is very low (1.3% in recent Society of Thoracic Surgeons congenital database analysis1). Potential complications that are specific to TOF surgery include RV dysfunction (usually limited), atrioven- tricular block (o3%), junctional ectopic tachycardia (o5%), patch dehiscence with residual VSD (poorly tolerated), and residual RVOT obstruction. Long-term outcomes are gene- rally excellent
- 157. • The pulmonary valve anatomy, as it relates to surgery, has been neglected. Z scores are simply normalized values of pulmonary annuli and do not reflect the degree of cusp dysplasia or effective orifice available. Thus, relying only on z scores can be misleading. Z scores need to be part of the overall picture, but intraoperative inspection of the valve is equally important. It is important to think in terms of valve morphology, not annular size
- 158. • Figure 1 After median sternotomy or partial lower sternotomy, a pericardial well is established. The heart is inspected from the outside, and typically there is a large size discrepancy between the ascending aorta and the main pulmonary artery (PA), as well as occasionally a “dimple” seen on the RVOT. The location of the coronaries is noted, knowing that in TOF, the right coronary artery origin is rotated leftward and is usually close to the MPA. The edges of the infundibulum are marked with 4-0 silk mattress stay sutures. The LAD denotes the septum, and the lateral stay sutures are placed several millimeters away from the LAD. A fine polypropylene suture is place to mark the exact middle of the PA bifurcation, for future orientation when making the main PA incision. A patent ductus arteriosus, if present, is ligated or clipped. SVC = superior vena cava; Ao = aorta; RAA = right atrial appendage; LAD = left anterior descending; RV = right ventricle.
- 159. •
- 160. • Figure 2 The aorta, SVc, and inferior vena cava are cannulated, and the patient is placed in mildly hypothermic cardiopulmonary bypass (32- 341C). The aorta is cross clamped, cardioplegia is delivered into the aortic root, and attention paid to a prompt diastolic arrest. The caval tapes are snared, a right atriotomy is performed, and a left ventricle vent placed though the PFO. The intracardiac anatomy (VSD, RVOT muscle bundles) is inspected. After control of the branch PAs, the MPA is incised longitudinally using the previously placed distal midpoint suture as a guide (it is easy to veer toward the LPA and thus create a problem at the distal MPA). If a decision has been made to make an infundibular incision, the RVOT is opened over approximately 1 cm at the point of greatest stenosis. RPA = right pulmonary artery; LPA = left pulmonary artery; VSD = ventricular septal defect.
- 161. •
- 162. • Figure 3 The VSD is closed via the infundibulum or the tricuspid valve using a patch with 5-0 Tevdek mattressed pledegted sutures (Fig. 3B). Care must be taken to avoid the inferoposterior edge to avoid the conduction system. Specific attention must be paid to the ventriculo- infundibular fold as this can be the site of troublesome intramural residual VSDs. The PFO is downsized to the desired size (typically 2-3 mm) with a polypropylene suture. Obstructing RVOT muscle bundles are excised. PFO = patent foramen ovale; VSD = ventricular septal defect
- 163. •
- 164. • Figure 4 Attention is now directed toward the RVOT and pulmonary valve. The pulmonary valve is inspected and the number of cusps, their consistency, the level of fusion, thickness, and the depth of the sinuses of Valsalva are noted. A Hegar dilator is passed to measure the effective orifice, NOT to dilate the valve. The cusps are thinned out gently, and each commissure is incised with a no. 15 scalpel blade down to the medial layers. Measure of the new effective orifice is now done again with Hegar dilators. These maneuvers usually gain an additional 1-2 mm in effective orifice diameter. Depending on the theoretical pulmonary annular size in relation to the body surface area, a decision is made about whether to stop or proceed with balloon dilation or pulmonary valve patch augmentation. A rough estimate is that if the effective orifice is within 1 mm of expected effective orifice for body surface area, nothing else is done. If the effective orifice is o2 mm from expected, slow and deliberate hand-controlled balloon dilation (Fig. 5) using as a first balloon diameter the size of the orifice measured after sharp commissurotomy. If the orifice is considered too small and an incision across the pulmonary annulus is deemed necessary, then patch augmentation of the pulmonary valve by division of the pulmonary annulus and anterior cusp in the midline, using the 2 divided halves of the anterior cusp to anchor the patch, is done (Fig. 6). PA = pulmonary artery.
- 166. • Figure 5 If one is in the middle range of z scores (typically around 2) and after commissurotomy and valve thinning the effective orifice should be expanded by another 2-3 mm, intraoperative balloon dilation is a good choice. This strategy is based on several theoretical advantages and experience with transcatheter pulmonary valvuloplasty in animals and humans. A balloon can be introduced across the valve annulus at a diameter much smaller than the orifice and then expanded. Dilation occurs in static position, and the radial transmission of stress imparted by the balloon allows for splitting of commissures as well as dilation and stretching of the annulus.10,11 The first balloon size should be the same size as the measured effective orifice after commissurotomy. One can then incrementally increase the balloon size by 1 mm. The balloons are dilated by hand under direct vision. PV = pulmonary valve
- 167. •
- 168. • Figure 6 Once a decision has been made to divide the annulus, both RVOT and PA incisions are joined. Most TOF pulmonary valves have a well-developed anterior cusp that is in the sagittal plane. That cusp is divided in the midline (Fig. 7). The tethering of the anterior cusp to the MPA is left untouched to preserve hinge function of the newly created large anterior cusp. If the patient has a commissure in the anterior midline, then the incision is made through that commissure. MPA = main pulmonary artery
- 172. Figure 9 That patch is sutured starting at the edge of the divided anterior cusp, leaving 1-2 mm protruding over the free edge of the valve, and anchoring the patch to the endothelial layers of the RVOT incision to create a pseudo sinus of Valsalva. RVOT = right ventricular outflow trac
- 174. Figure 10 Another oval-shaped Cormatrix patch is sutured from the distal main PA to the RVOT covering the entire incision. The right atrial incision is closed after ensuring that there is no tricuspid regurgitation. The patient is weaned off bypass per routine protocol. Pacing wires are placed if any evidence of rhythm problem exists
- 177. Figure 1. A: fan- shaped expanded polytetrafluoroethyl ene (PTFE). B: suturing the vertex of the patch (A) and central point of the curved edge (B). C: suturing both straight edges of the patch to those of the ventriculotomy incision (C,D). D: transannular patch of autologous pericardium (covering the PTFE valve).
- 182. Figure 4 Patch augmentation of the pulmonary artery. The bovine pericardial patch is trimmed (A). The patch is sewn onto the main pulmonary artery using 4-0 prolene running suture (B). In case the patient has a branch pulmonary stenosis, patch augmentation is performed prior to main pulmonary artery plasty.
- 184. Figure 6 The bioprosthesis is then sewn onto the pulmonary annulus using 4-0 prolene running suture
- 185. Figure 7 After completing the suturing of the bioprosthesis on the posterior side, the suture is brought outside of the pulmonary artery and tied with the suture used in the bovine pericardial patch for pulmonary artery.
- 186. Figure 8 The anterior aspect of bioprosthesis is now sewn to the bovine pericardial patch using 4-0 prolene suture
- 188. Figure 10 Patching right ventricular outflow tract. The incision of the right ventricular outflow tract is augmented with the same bovine pericar- dium used in the pulmonary artery. The right ventricular outflow tract should be augmented so that it does not cause subvalvular stenosis. This is especially important when using a large-size bioprosthesis (ie, >25 mm) to prevent size mismatch between pulmonary annulus/right ventricular outflow tract and bioprosthesis. The choice of valve size is based on the surgical strategy used at each institution. Our strategy is to consider the potential future “valve-in-valve” procedure when the implanted bioprosthesis may have deteriorated; therefore, we pick a valve greater than 29 mm in size. Patients with significant pulmonary regurgitation have a decreased and dilated right ventricle (RV) with very thin right ventricular outflow tract (RVOT). We believe that a ventriculotomy in these patients does not impact RV function. Rather, we rather con- sider future re-intervention, especially in adolescent patients. Not utilizing a ventriculotomy results in a smaller valve being implanted, such as 23 or 25 mm. In such cases, hypertrophied muscle has often been seen in the RVOT, which also leaves a significant outflow gradient
- 190. Figure 11 Comparison of aortic and 29 mm mitral bioprosthesis. The length from the cuff to the top of the valve (the supravalvular part of bio- prosthesis) is lower (ie, low profile) in the mitral compared to the aortic (9 mm vs 11 mm). This smaller size is important to ensure the stent posts do not interfere with the bifurcation of the pulmonary artery, which could result in branch pulmonary artery stenosis. The cuff is thicker in the mitral compared to the aortic (4 mm vs 2 mm), which makes it physically easier to implant the bioprosthesis. Other than these features, the basic structure is not different between the aortic and the mitral bioprosthesis. We routinely use the porcine bioprosthesis, although it is generally believed that there are no differences between bovine and porcine valves regarding future intervention. Because of its material charac- teristics, we think bovine pericardium is suitable for patients with pulmonary hypertension or pulmonary stenosis as they may require catheter assessment/treatment later. Porcine valve is thinner and it bears a risk of leaflet injury when the catheter is passed through the valve. For future “valve in valve” procedure, we recommend the implantation at the anatomical position (ie, true annulus). The implantation at supravalve may cause the compression of the left coronary artery and hence not recommended
- 192. Conclusion Pulmonary valve replacement is now gaining the greatest population in surgical treatment for adult congenital heart disease. We demonstrated the technique of implantation of bioprostheis in patients having pulmonary regurgitation and/ or stenosis. There are several choices of techniques and the prosthetic valve, and the best way to obtain the best long- term outcome has still not been elucidated. One of the prob- lems of using a bioprosthesis is its relatively short lifespan, therefore, the need for potential future reintervention should be considered at the time of pulmonary valve replacement.
- 193. Tetralogy of Fallot with Pulmonary Stenosis
- 198. Tetralogy of Fallot with Pulmonary Atresia
- 199. Figure 37-2 the specimen shows the phenotypic features of tetralogy of Fallot, in that the deviated outlet septum is attached antero-cephalad relative to the limbs of the septo-marginal trabeculation (yellow Y). In this heart, however, there is muscular subpulmonary (pulm.) atresia, rather than pulmonary stenosis. note also the muscular postero-- inferior (post.-inf.) rim to the interventricular communication
- 200. Figure 37-3 In this example, the atresia is produced by an imperforate pulmonary valve. note again the abnormal insertion of the outlet septum (star) relative to the septo-marginal trabeculation (yellow Y).
- 201. Figure 37-4 In this heart, the pulmonary trunk is represented by a fibrous strand, but the strand takes its origin from the right ventricle. the aortic valve is attached directly to the parietal ventricular wall, with no evidence of the subpulmonary infundibulum. the yellow Y shows the septo-marginal trabeculation
- 202. Figure 37-5 In this example, the deviated outlet septum is no more than a fibrous raphe, and there is an imperforate pulmonary valve. this is tetralogy of Fallot with pulmonary atresia in the setting of a doubly committed and juxta-- arterial interventricular communication. note the position of the septo-marginal trabeculation (yellow Y ).
- 203. Figure 37-6 In this heart, there is obvious deviation of the outlet septum (star) relative to the septo-marginal trabeculation (yellow Y ), with muscular pulmonary atresia, and a perimembranous interventricular communication. note the fibrous continuity between the leaflets of the aortic and tricuspid (tric.) valves, and the seagull configuration of the pulmonary arteries
- 209. Tetralogy of Fallot with Pulmonary Atresia (Pulmonary Atresia and Ventricular Septal Defect) Prevalence Pulmonary atresia occurs in about 15% to 20% of patients with TOF.
- 210. Pathology 1. The intracardiac pathology resembles that of TOF in all respects except for the presence of pulmonary atresia, the extreme form of RVOT obstruction. The atresia may be at the infundibular or valvular level. 2. The PBF is most commonly mediated through a PDA (70%) and less commonly through multiple systemic collaterals (30%), which are referred to as multiple aortopulmonary collateral arteries (MAPCAs). Both PDA and collateral arteries may coexist as the source of PBF. 3. The central PAs are usually confluent in patients with PDA (70%). In patients with MAPCAs, the central PA is frequently nonconfluent, with the right upper lobe frequently supplied by a collateral from the subclavian artery and the left lower lobe by a collateral from the descending aorta. The subgroup of the patients with MAPCAs is designated as pulmonary atresia and ventricular septal defect (PA-VSD).
- 211. 4. PA anomalies are common in the form of hypoplasia, nonconfluence, and abnormal distribution. a. The central PAs are confluent in 85% of patients; they are nonconfluent in 15%. b. b. The central and branch PAs are hypoplastic in most patients, but this occurs more frequently in patients with MAPCAs than in those with PDA. The degree of PA hypoplasia is importantly related to the success of surgery (see below for further discussion of PA hypoplasia. c. c. Incomplete arborization (distribution) of one or both PAs is found in 50% of patients with confluent PAs and in 80% of patients with nonconfluent PAs.
- 212. 5. Collateral arteries arise most commonly from the descending aorta (occurring in two thirds of patients), less commonly from the subclavian arteries, and rarely from the abdominal aorta or its branches. 6. The ductus is small and long and arises from the transverse aortic arch and courses downward (“vertical” ductus) (Fig. 14-25).
- 214. 7. The McGoon ratio and the Nakata index are used to quantitate the degree of PA hypoplasia. Small values of these measurements may adversely affect the outcome of surgeries in patients with small pulmonary arteries. a. The McGoon ratio is the ratio of the sum of the diameter of the immediately prebranching portion of the RPA plus left pulmonary artery (LPA) divided by the diameter of the descending aorta just above the diaphragm. Normal values of the McGoon ratio are 2.0 to 2.5. Most survivors of TOF with pulmonary atresia have a ratio greater than 1. Good Fontan candidates should have a ratio greater than 1.8.
- 215. b. The Nakata index is the cross-sectional area of the RPA and LPA (in mm2) divided by the body surface area (BSA). The average diameter of both RPA and LPA are measured at the points immediately proximal to the origin of the first lobar branches at maximal and minimal during one cardiac cycle in the anteroposterior view of the pulmonary arteriogram. The cross-sectional area is calculated by using the formula, π × r2 × magnification coefficient (where r is the radius or 1/2 of the measured PA diameters). A normal Nakata index is 330 ± 30 mm2/BSA. Patients with TOF with PS should have an index greater than 100 for survival. A good Fontan candidate should have an index greater than 250, and a good Rastelli candidate should have an index greater than 200. (Those with an index less than 200 should have a shunt operation rather than the Rastelli.)
- 216. Clinical Manifestations 1. These patients are cyanotic at birth. The degree of cyanosis depends on whether the ductus is patent and how extensive the systemic collateral arteries are. 2. Usually a heart murmur cannot be heard. However, a faint, continuous murmur may be audible from the PDA or collaterals. The S2 is loud and single. A systolic click is occasionally present. 3. The ECG shows RAD and RVH. 4. Chest radiography shows a normal heart size. The heart often appears as a boot-shaped silhouette (see Fig. 14-19), and the pulmonary vascularity is usually markedly decreased (i.e., “black” lung field). Rarely, children with MAPCAs have excessive PBF, and CHF may develop.
- 217. 5. Echocardiographic studies show all the anatomic findings of TOF plus the absence of a direct connection between the RV and the PA. In this case, a careful examination of the central PA is necessary with measurements of the size of central and branch PAs. The small branch PAs and “vertical ductus” (see Fig. 14-25) are well imaged from a high parasternal or suprasternal transducer position. Some of the multiple collateral arteries are also imaged by echocardiography and Doppler
- 218. 6. Cardiac catheterization and angiograms are sometimes needed for a complete delineation of the collaterals. Alternatively, MRI, rather than CT, is chosen for complete anatomic delineation of the aortic collaterals and PA branches.
- 219. Natural History 1. Without immediate attention to the establishment of PBF during the newborn period, most neonates who have this condition die during the first 2 years of life; however, infants with extensive collaterals may survive for a long time, perhaps for more than 15 years. 2. Occasionally, patients with excessive collateral circulation develop hemoptysis during late childhood.
- 221. Surgical A connection must be established between the RV and true PA as early in life as possible. This may allow tiny central PAs to enlarge rapidly during the first year of life with improved arborization (distribution) of the pulmonary arteries with concurrent development of alveolar units. To achieve this goal, some centers initially use a central shunt procedure, and others proceed with an RV–PA connection
- 222. 1. Central shunt operation. Some centers use a central shunt directly connecting the ascending aorta and the hypoplastic main PA to achieve growth of the peripheral PAs (Mee procedure) (Fig. 14-26).
- 223. VSD+Pulmonary atresia+Hypoplastic pulmonary arteries MPA is transected at the right ventricular end and clamped. Pulmonary blood flow is maintained by patent ductus arteriosus.
- 226. Modified Mee Shunt Modified Mee Shunt is an aortopulmonary central shunt developed in 2012 by Dr.Bugra HARMANDAR for the palliation of newborns with ventricular septal defect (VSD), pulmonary atresia and very hypoplastic pulmonary arteries.
- 227. 2. RV-to-PA connection a. Single-stage repair. Complete, primary surgical repair in patients with TOF and pulmonary atresia is possible only when (1) the true PAs provide most or all PBF (with O2 saturation of >75%) or (2) (2) the central PA connects without obstruction to sufficient regions of the lungs (i.e., at least equal to one whole lung). If additional major collaterals are identified, test the level of arterial O2 saturation after occlusion of the collateral in the catheterization laboratory. If the O2 saturation remains greater than 70% to 75%, coil occlusion of the collaterals is then carried out.
- 228. Primary repair of this condition consists of closing the VSD, establishing a continuity between the RV and the unifocalized PA (see below for unifocalization procedure) using either aortic or pulmonary homograft (9- to 10-mm internal diameter), and interrupting collateral circulation. The mortality rate varies between 5% and 20%. Good candidates for the repair are those with a Nakata index above 200. If the index is below 200, a shunt procedure is preferable.
- 229. b. Multiple-stage repair. When the requirements for single-stage repair are not met, three consequential steps are used to repair this condition. These steps are summarized in Figure 14-27. (1) Stage 1. RV-to-hypoplastic PA conduit, using a relatively small homograft conduit (6- to 8-mm internal diameter) (see Fig. 14-27). The major goal of this operation is to make the central PA grow to an adequate size for eventual repair surgery. Interventional catheterization is carried out 3 to 6 months later to identify and coil occlude remaining aortic collaterals, to define PA distribution, and to identify if certain bronchopulmonary segments are receiving a duplicate blood supply. (2) Stage 2. A unifocalization procedure is carried out. Unifocalization is a surgical procedure in which aortopulmonary collaterals are divided from their aortic origin and are anastomosed to the true pulmonary arteries or main PA conduit (see Fig. 14-27)
- 230. Post-unifocalization catheterization is carried out 3 to 6 months later (a) to identify multiple peripheral stenosis in both the true as well as the unifocalized collaterals and to do balloon dilatation with or without stenting and (b) to assess the need for further unifocalization procedures. (3) Stage 3. Closure of VSD with or without fenestration, usually at 1 to 3 years of age (see Fig. 14-27). The homograft conduit may need to be replaced at the same time. If the RV pressure is 10% to 20% greater than systemic pressure, a central fenestration 3 to 4 mm is created. Multiple ballooning and stenting procedures are often necessary to reduce RV pressure to less than 50% systemic if possible.
- 233. FIGURE 14-27 Diagram of multiple-stage repair. Upper row (confluent pulmonary artery [PA] and collaterals): A, A hypoplastic but confluent central PA and multiple other collateral arteries are shown. B, A small right ventricle–to–PA (RV-to-PA) connection is made with pulmonary homograft (shown shaded), with collaterals left alone. C, The pulmonary arteries have grown to a larger size, and a larger pulmonary homograft has replaced the earlier small one. Collateral arteries are now anastomosed (unifocalized) to the originally hypoplastic PA branches. The ventricular septal defect (VSD) may be closed at a later time usually 1 to 3 years of age. The pulmonary homograft is usually replaced with a larger graft at this time. Bottom row (nonconfluent PA and multiple collaterals): A, Absent central PA and multiple aortic collaterals are shown. B, A small pulmonary homograft (6–8 mm internal diameter, shown shaded) is used to establish the RV-to-PA connection with some collaterals connected to it (unifocalized) (performed at 3–6 mo). Some collaterals are not unifocalized at this time. C, The homograft conduit has been replaced with a larger one. Remaining collateral arteries are anastomosed to the pulmonary homograft to complete unifocalization procedure. The VSD is closed with or without fenestration, usually at 1 to 3 years.
- 242. Right Ventricle–to–Pulmonary Artery Conduit Figure 12-3 A An incision is made into the confluent portion of the pulmonary artery. If necessary to achieve adequate length, the incision is extended onto the left pulmonary artery.
- 243. B The distal end of a prosthetic valved conduit is shortened to a point just above the heterograft valve. The conduit shown here is meant to be generic; valves from a variety of species have been employed. The composite valved conduit is approximated to the pulmonary artery by continuous suture. To ensure accurate closure, several suture loops are placed around the apex of the incision onto the left pulmonary artery before the prosthesis is pulled into the arteriotomy. Generous bites of tissue are taken in each stitch, including as much of the overlying pericardial tissue as possible to strengthen the anastomosis and ensure a tight tissue-to-graft approximation. The pulmonary artery is often thin and fragile, making it extremely important to use accurate suture technique and follow the arc of the needle precisely. Low-flow cardiopulmonary bypass or short periods of circulatory arrest, which reduce the amount of blood in the pulmonary artery due to aortopulmonary collateral flow, are useful to achieve optimal visualization of the anastomosis. The suture line is continued in a counterclockwise fashion about halfway around the anastomosis
- 245. C The suture line is completed in a clockwise fashion anteriorly. Placing the valve portion of the conduit close to the pulmonary artery avoids compression of either the valve or the surface coronary arteries. D The proximal end of the composite conduit is shortened and beveled for approximation to the right ventriculotomy. A continuous stitch of 4/0 polypropylene is used to anastomose the conduit to the surface of the right ventricle. Several suture loops are placed at the heel of the conduit to ensure accurate approximation. E The suture line is taken in a counterclockwise fashion to the right lateral margin of the ventriculotomy. The anastomosis of the conduit to the surface of the right ventricle is completed in a clockwise fashion around the toe of the valved conduit. Several interrupted pledget-reinforced mattress stitches are placed to reinforce the anastomosis if the branch pulmonary arteries are small or if there is evidence of obstructive pulmonary vascular disease, which will likely result in high postoperative right ventricular pressure
- 248. F Allograft tissue can be used for the conduit. Both aortic and pulmonary allografts have been used for this purpose, but the pulmonary allograft may be preferred because of its favorable anatomic structure. The graft usually consists of a portion of the outflow tract of the right ventricle, the pulmonary valve, and the pulmonary artery, including the right and left branches. The myocardium of the outflow tract is trimmed, leaving the scalloped pulmonary valve hinge point (“annulus”). A polytetrafluoroethylene (PTFE) graft of appropriate size is fashioned to match the scallop of the pulmonary valve and is attached by continuous suture to the pulmonary allograft. An externally reinforced graft can be used if there is concern that anterior chest call compression might occur after repair. The pulmonary artery bifurcation is opened by incision of the superior aspect between the right and left branches of the pulmonary artery.
- 252. Tetralogy of Fallot with Absent Pulmonary Valve Prevalence Tetralogy of Fallot with an absent pulmonary valve occurs in approximately 2% of patients with TOF
- 253. Pathology and Pathophysiology 1. The pulmonary valve leaflets are either completely absent or have an uneven rim of rudimentary valve tissue present. The annulus of the valve is stenotic and displaced distally. A massive aneurysmal dilatation of the PAs is present. This anomaly is usually associated with a large VSD, similar to that seen in TOF. It rarely occurs with an intact ventricular septum.
- 258. Natural History 1. More than 75% of infants with severe pulmonary complications (e.g., atelectasis, pneumonia) die during infancy if treated only medically. The surgical mortality rate of infants with pulmonary complications is 20% to 40%. 2. Infants who survive infancy without serious pulmonary problems do well for 5 to 20 years and have fewer respiratory symptoms during childhood. They become symptomatic later and die from intractable right-sided heart failure.
- 259. Management Medical In the past, medical management was preferred because of poor surgical results in newborns; however, the mortality rate of medical management is much higher than surgical management. After the pulmonary symptoms appear, neither surgical nor medical management has good results.
- 260. Surgical Symptomatic neonates should have corrective surgery on an urgent basis. Even asymptomatic children should have elective surgery in the first 3 to 6 month of life.
- 261. Primary Repair Complete primary repair is the procedure of choice. VSD is closed through right ventriculotomy (across the pulmonary annulus). In symptomatic neonates, a pulmonary homograft is used to replace the dysplastic pulmonary valve and the dilated main and branch PAs. Alternatively, a valved conduit may be used to restore competence of the pulmonary valve, and the aneurysmal PAs are plicated. Some surgeons advocate aortic transection to achieve good exposure of the PAs for an extensive pulmonary arterioplasty into the hila of both lungs. An early surgical mortality rate is as high as more than 20% with a 1-year survival rate of 75%.
- 262. Figure 1 The chest is entered through a median sternotomy and the thymus gland is removed. The pericardium is opened and a portion is harvested and placed in glutaraldehyde for later use. Examination of the external cardiac anatomy shows the main pulmonary artery to be slightly enlarged and the right and left pulmonary arteries to be quite dilated, equal to or larger in size than the aorta. The segmental branches of these vessels are small. For larger patients we utilize aorto-bicaval cannulation and continuous cardiopulmonary bypass. For smaller patients, especially those with small superior venae cavae, we place aortic and right atrial cannulae. The patient is then cooled to 18°C. During cooling, the branch pulmonary arteries are mobilized out to the hilar branches. The aorta is then cross-clamped and 30 mL/kg of cold blood cardioplegia is administered via the aortic root. We then perform the operation under circulatory arrest with 2-minute periods of intermittent perfusion every 15 minutes. Additional doses of cardioplegia are given at these times as well.
- 266. Figure 4 (A, B) The ventricular septal defect is closed with a Gore-Tex patch. A combination of plegeted, in- terrupted sutures and non-plegeted running prolene sutures are used. The plegeted sutures are used along the base of the septal leaflet of the tricuspid valve and the running su- tures for the remainder of the clo- sure. The sutures are kept on the right side of he septum in the region of the bundle of His in order to min- imize the chance of heart block.
- 273. Figure 10 An appropriate sized pulmonary homograft is anatamosed to the pulmonary artery reconstruction distally using a running prolene suture. During this time, the patient is rewarmed and at the completion of the suture line, the left side of the heart is deaired and the aortic cross clamp is remove
- 277. Figure 2 After clamping the aorta and delivering of cardioplegia, a short (10-15 mm) transannular longitudinal incision is made in the right ventricular outflow tract. The parietal band is transected to enlarge the right ventricular outflow tract. PA pulmonary artery; RV right ventricle; VSD ventricular septal defect
- 278. Figure 3 (A) If the parietal band is properly divided, a transatrial approach offers very good exposure for the closure of the ventricular septal defect, even in neonates. If necessary, extended resection of right ventricular outflow tract can be accomplished working through the tricuspid valve as well. (B) A continuous suture technique and Dacron patch are preferred. Alternatively, in neonates with a very fragile myocardium, a pledgeted suture technique should be used. The foramen ovale in newborns and small infants is left open. TV tricuspid valve; VSD ventricular septal defect. (Redrawn from Bove.)
- 279. Figure 4 The transverse aortotomy is performed above the aortic valve commissures. A short tubular segment of the aorta is resected. This maneuver brings the future ascending aorta down and to the left. Resection of aorta, especially in newborns, might be omitted, to avoid too close a relationship between the aorta and the trachea and left bronchus.
- 280. Figure 5 The pulmonary artery is transected above the annulus. Care is taken to stay away from left coronary artery. If the left pulmonary artery is too long, the pulmonary trunk is obliquely cut toward the left pulmonary artery. LCA left coronary artery; LPA left pulmonary artery; RPA right pulmonary artery.
- 281. Figure 6 The transected pulmonary artery is mobilized, if necessary, and brought anterior to the aorta. At this point, end-to-end anastomosis of the ascending aorta is performed. Care is taken not to compress the right coronary artery by the translocated pulmonary artery. In particular, the right pulmonary artery must be mobilized adequately to avoid undue tension on the right coronary artery.
- 282. •
- 283. •
- 284. •
- 285. •
- 286. •
- 287. •
- 288. Postoperative Management in ICU