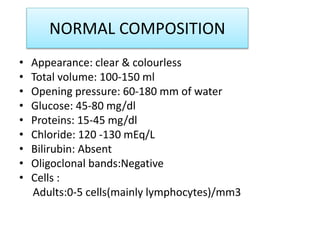
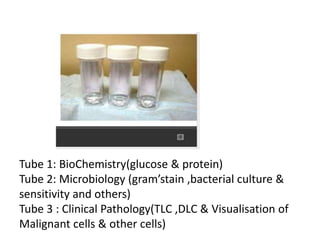
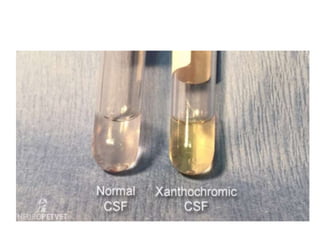
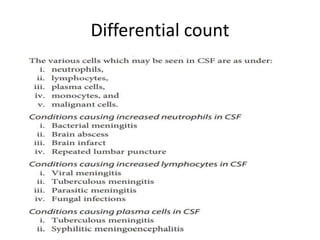
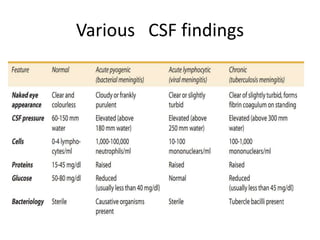
CSF analysis provides important diagnostic information for conditions affecting the central nervous system. CSF is collected via lumbar puncture and analyzed for opening pressure, appearance, chemistry including glucose and proteins, cell counts and differentials, and microbiology. Abnormal findings can indicate infections like meningitis, tumors, hemorrhages, and other CNS pathologies. A thorough CSF analysis incorporating results from biochemistry, hematology, and microbiology departments helps reach the correct diagnosis and guides patient management.