3. Definition
• A fracture is a disruption in the continuity of a
bone stressed beyond its elastic modulus, with
the formation of two or more fragments.
4. I. Location of problem to be treated.
II. Diagnosis & treatment plan
III. Documentation
IV. Assessment of treatment
V. Epidemiological studies
5. • Direct or indirect
• Complete or incomplete
• Mechn- bending, torsion, shear, contrecoup. avulsion and
burst type
• Site
• Displacement
• Number-single ,multiple or comminuted
• Integument- closed or open
• Shape- transverse ,oblique butterfly,
• oblique surface fracture
10. 1. Number of fracture /fragments ( F)
2. location of fracture ( L)
3. Status of occlusion (O)
4. Soft tissue involvement (S)
5. Associated injuries (A)
11. • F0- Incomplete fracture
• F1- Single fracture
• F2-Multiple fracture
• F3-Comminuted fracture
• F4-Fracture with a bony defect
18. • S0-closed
• S1-open intraorally
• S2-open extraorally
• S3-open intra and extraorally
• S4-soft tissue defect
19. • A0-None
• A1-Fracture or loss of tooth
• A2-Nasal bone
• A3-Zygoma
• A4-Le Fort I
• A5-Le Fort II
• A6-Le Fort III
20.
21. • Three stages-
Immediate assessment and treatment of any condt
constituting a threat to life
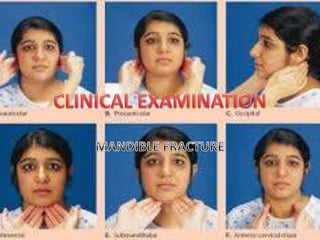
General clinical examination
Local examination
22. • Mf injuries may associated with body injuries may constitute threat to life
than facial trauma
• Rapid survey & Assessment
A-Airway
B-Breathing & Ventilation
C-Circulation & Hemorrhage control
D-Disability-Neurological assessment
E-exposure to external environment
27. • Recognition
Central pulse –Femoral /carotid
Skin colour-pink-ashen grey-white
Level of consciousness-confusion-aggression-drowsiness-
coma
Pulse- 120/min ( very thready)
Respiratory rate-20/min- Tachypnea
Weakness-due to hypoxia ,acidosis
Urinary out put- >30 ml/hr- 0-10 ml/hr
28. • Fluid replacement- Crystalloids. Colloids, Blood
• Local-( Maxillofacial aspect)
Pressure pack
Ligation of Vessel
Direct dental wiring at fracture region
29.
30.
31. • Careful clinical examination and no operative intervention
without rule out additional more serious injuries
• If cerebral hemorrhage , loss of consciousness
• Additional injuries required urgent treatment than MF injuries
• In polytrauma pt treated concurrently
• Major injuries- careful inspection/palpation reveal their
presence –treated accordingly
32. • If fracture mandible pt in
shocked, very unusual,
• Some more serious
condition other than
fracture mandible should be
suspected and treated
• first
33.
34. • Preparation for examination
• Face-gently cleaned with warm water
• Remove road dirt etc-evaluation of soft tissue injury
• Mouth-loose ,broken teeth,or dentures,any congealed blood
removed with swab in nontooth forcep
• If denture-full/ pieces reassemble piece so portion should be
missing-possibly displaced down into throat
• Complete extra & intra oral cleaning-assess full extent of injury
35. • During cleaning cranium and cervical spine should be carefully
inspected and palpated for sign of injury
36. Extravsation of blood from
injured bone resulted swelling
of face-more swelling increase
capillary permeability and
edema
Swelling+ecchymosis-fracture
Facial deformity-fracture &
displaced fragment
Open hang mouth-B/L condylar
#
37.
38. • Conscious pt- support his jaw with own hand
• Compound fracture- blood stained saliva may dribbled out from
corner of mouth
• Palpation-begin from bilateral condylar region-
downwards posterior along lower border of mandible.
• Any bone tenderness- pathognomic of fracture
• Deformity /bony cerpitus present
• Anesthesia/ paresthesia- injury to IAN- reduced or absent sensation
On one or both side of the lower lip
39.
40.
41.
42. Intra Oral Examination
Clean oral cavity-lukewarm mouth
wash/ cleaned with moistened
swab
Congealed blood,fragments of
tooth,alveolus,denture removed
with forcep/ suction tip
Buccal & Libgual sulci-
ecchymossis,submucosal
extravastion of blood-#
43. • Any lingual mucosa hematoma-#
• Bec lingual mucosa directly overlied periosteum of mandible
• Linear hematoma in third molar reg-indi fracture
44.
45. Edentoulus/ alv ridge
Step in occlusion,laceration in
overlying mucosa
Tooth-
luxation/subluxation,crown
fracture/dentine/pulp exposed ?
Any loose filling,fine crack/split
tooth
Missing-tooth,f illing, crown,
denture, portion of tooth-
CHEST X-RAYS
46. • Fracture site- mobility placing
finger and thumb on each side
and using pressure to elicit
mobility
• Any pain in jaw movement
recorded.
• Flat of both hands placed over
two angles of mandible and
gentle pressure exerted-if pain
• If crack fracture is present
48. • Direction and intensity of the traumatic force.
• Site of fracture
• Direction of fracture line
• Muscle pull exerted on the fractured fragments
• Presence or absence of tooth.
• Extent of soft tissue wounds
50. Injury
Pain- pain upon movement r remote from the site of injury
Abnormal mobility-abn mobility in dental arches r during jaw
movement.
Bleeding- active bleeding / hematoma or ecchymosis may
follow a fracture process.
Crepitus- Cracking, grating sound can be detected during
palpation of injury site.
51. Deformity-facial deformity depending upon degree and
direction of impact, also direction of fracture line and muscle
pull also.
Ecchymosis- and edma- seen extra orally and intraorally
depending upon impact and site of fracture.
Loss of function or interference with function-Mastication
problem, speech and difficulty in swallowing.
52. • Paresthesia/ hypoesthesia of lower lip- fracture between
mental foramen and ramus region
• Radiographic evidence-all suspected cases must be
radiographed. help as diagnostic aid and addition
confirmation also for medico legal documentation and as
evidence.
54. • Dento alveolar
• Condylar
• Coronoid Process
• Ramus
• Angle
• Body
• Symphysis & para symphysis
• Comminuted fracture
Anatomical
55. • Avulsion/subluxation or fracture of tooth in
association with fracture of alveolus.
• DA fracture alone
• DA plus mandibular fracture
56. • Laceration, full thickness wound of lower lip-imp low
teeth
• complete loss of soft tissue
• Bruising with embeded tooth portion/ foreign body
• Alv margin-laceration of gingiva, deformity of alveolus
• Degloving injury
57.
58. • Impaction of point of chin on some resilient surface-soft earth
• Jaw does not fracture but soft tissue rotated violently over
point of chin. horizontal tear at junction of attached & free
gingiva
59. • Tooth- lost, recent extn wound-knocked out
• Split/ Fracture- premolar & Molars- horizontal / vertical split
below the gingival margin-indirect trauma from opposing
dentition
• Crown- fracture, embedded into soft tissue, swallowed or
inhaled.
60. • If pulp/near pulp exp-immediate treatment
• Root- fracture, excessive mobile tooth, subluxated ?
• IOP Xrays
• Thermal sensitivity-unreliable to test injury to pulp
• Trauma/ force –disturb the function of nerve endings
61. • Isolated fracture
• With injury to tooth
• Gross comminution of Alveolus
• Alv fracture consists one or two fragments containing teeth
• Complete Alv Fr+ Teeth segment displaced into soft tissue of
the floor of mouth covered by mucosa.
•
62. • +-Difficult to differentiate alveolar fracture from symphysis
fracture-
• Unless palpate at lower border of mandible.
• During examn easy to reposition the alveolar fracture
fragment in position-better prognosis.
63. • Most common overall fracture ( 20 % )
• Easily missed fracture during examination
64. • Unilateral / Bilateral
• Intra capsular / Extra capsular( condylar Neck).
• Extra capsular type-with or without dislocation
65. • Inspection-
• Swelling over joint - +
• bleeding from ear( laceration of antr wall of EAM
• D/D-bleeding from middle ear +CSF otorrhoea- Petrus
temporal bone #
• Ecchymosis of skin below mastoid process-when hematoma
surrounding fractured condyle tracked down to EAM.
• D/D Battle Sign ( Base of Skull # )
• If mandible locked- when condyle impacted through glenoid
fossa
66. • If condyle medially dislocated-when edema subsided hollow
characteristic sign will be present
• Immediate post trauma-sign obscured by edema.
67. • Tenderness over condylar area
• EAM palpation –when condyle is dislocated from glenoid fossa.(standing
in front of pt both little can be hooked into each EAM ).
• Rarely hemorrhage from condylar region track across the base of skull-
exert pressure on mand. Divin. Of Vth N at F.Ovale-paresthesia of lower lip
• D/D-Fracture of Body / Angle region of mandible rule out
68. Condyle dislocated resulted
ramus height shortening-
Molar gagging of the occlusion.
Deviation of mandible towards fracture side.
Painful movements- Lateral excursion to
opposite side
-Protrusive movement .
69. • Extra orally- same sign & symptoms bilaterally
• Mandibular movement restricted.
• Intra orally-
• In intra capsular fracture bilaterally- if any ramal shortening but normal
occlusion.
• Extracapsular #- b/L condylar dislocation- B/L ramus shortening
/overriding of fracture fragments- Antr open bite.
• Painful & limited opening movements.
• Painful & restricted protusion n lateral excursions
70.
71. Guard man fracture- B/L condylar fracture with Symphy or
Parasymphysis fracture
72. • Rare fracture
• Result from reflux contracture of powerful antr fibres of
temporalis muscle.
• Direct trauma to ramus- # coronoid process
• Tip #-pulled upwards into infratemporal space ( Temp M )
• Sometime- surgery of cyst r large tumor of the ramus.
• Palp-tenderness over antr part of ramus, tell-tele hematoma
• Painful, limited protrusive movement.
73. • Not common- two types
• Single fracture- Low condylar fracture-both condyle &
coronoid process on upper fragment.
• Comminuted Fracture- direct violence from gun shot/missile
injury- fragments splinted between masseter muscle and
medial pterygoid muscles with little or no displacement.
74. Swelling & ecchymosis extra & intraorally.
Tenderness over the ramus .
Severe trismus present ?
75. • Inspection-
Swelling
Facial deformity
I/O step deformity behind last molar
Presence of hematoma Buccal r lingual side or both adjacent
to fracture.
Anesthesia or paresthesia of the lower lip.
Occlusion-deranged.
76.
77.
78. • Palpation-
Tenderness present at angle region
Movement /crepitus at fracture site ( if ramus steadied
between finger and thumb and body of mandible
moved gently with the other hand) .
Step may palpated.
Painful restricted jaw movements.
79. • Swelling
• Tenderness
• Displaced fractured fragment, causes derangement of occlusion
• Premature contacts in distal fragment (displacing action of muscles
attached to Ramus)
• Occlusion Derangement.
• Gingival tear due to its firm attachment -displaced fragments
80. • If gross displacement can
cause Intra oral
hemorrhage-IAA torned ?
• Molar & Premolar tooth-
split longitudinally /
vertically- considerable
discomfort
82. • Commonly associated with one /both condyle.
• Presence of bony tenderness & lingual hematoma important
sign-
• Bec antr mandible thickness between often ensure fine
cracks with little displacement.
• May be missed if occlusion is undisturbed locally.
•
83. Bony tenderness and small lingual hematoma may be only
physical sign present
Severe impact( direct violence-oblique fracture-displaced
fragments. Which allows over riding of the fragments with
lingual inversion of the occlusion on each side.
Always associated soft tissue injury of chin and lower lip
84. • Detachment of genioglossus M – may contribute loss of
tongue control.
• Airway obstruction.
• If Pt Conscious- voluntarily control of tongue
prevent obstruction.
• If unconscious- stay suture of tongue/airway
to prevent tongue fall.
• No paresthesia of skin of mental region unless
mental nerve is involved.
Editor's Notes
mobility placing finger and thumb on each side and using pressure to elicit mobility