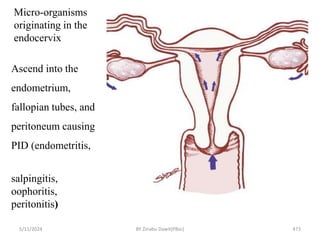
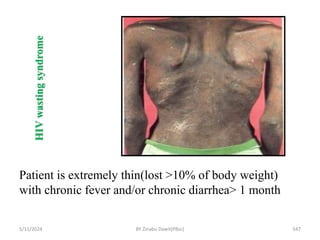
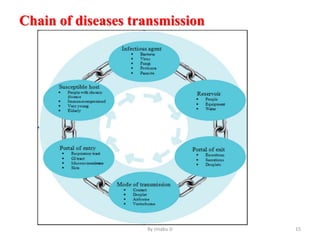
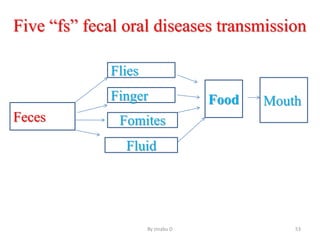
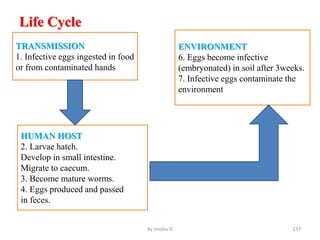
The document provides an overview of communicable diseases, including their definitions, transmission methods, and common terms associated with them. It details the chain of disease transmission involving infectious agents, reservoirs, portals of exit and entry, and susceptible hosts, along with preventive measures and levels of prevention. Specific examples of diseases such as typhoid fever and the fecal-oral transmission route are also discussed.

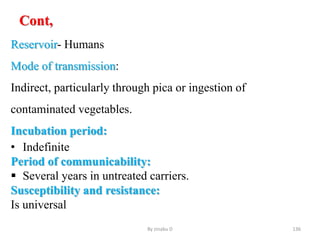

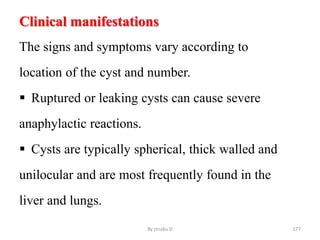

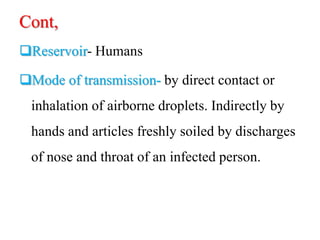
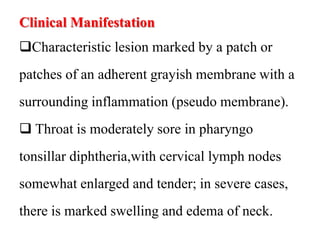

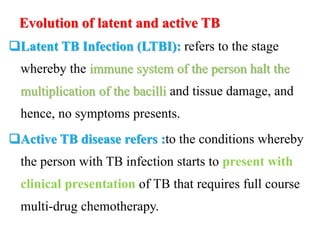





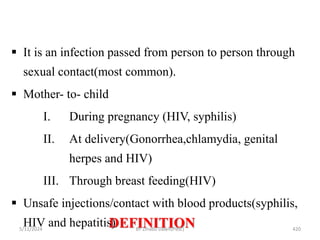

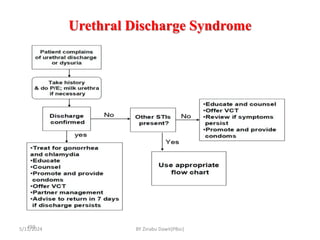
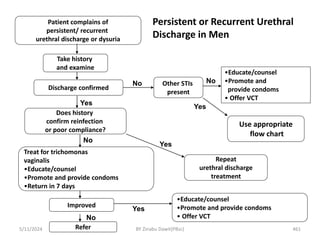
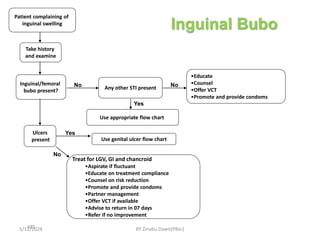
![complains of urethral discharge or dysuria
Take history & Examine [Milk urethra if necessary]
Discharge present? Other
STIs?
No
Yes
Use appropriate flow chart
Yes
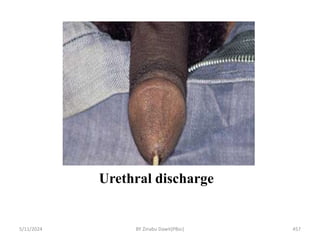
Urethral discharge
• Educate on RR
• Offer CTP
• Promote &
provide condoms
Treat for CT
•Educate on risk reduction
•Offer HCT
•Promote & provide condoms
• Partner management
• Advise to return in 7 days if symptoms persist
Figure 1
5/11/2024 460
BY Zinabu Dawit(PBsc)](https://image.slidesharecdn.com/communicabledisease-240511200424-c396173f/85/Communicable-Disease-pptxgfgfggfffdfxfsdddf-460-320.jpg)