Dentist in pune.(BDS) MDS- OMFS - Dr. Amit T. Suryawanshi.. Mandibular fractu...All Good Things
Dentist in pune. (BDS. MDS) - Dr. Amit T. Suryawanshi. Seminar-Canine Impaction.
Email ID- amitsuryawanshi999@gmail.com
Contact -Ph no.-9405622455
Subscribe our channel on youtube - https://www.youtube.com/channel/UC_gylEXTrjmEbbOTSXjuZ4Q/videos?view_as=public
Follow us on slideshare
Dentist in pune.(BDS) MDS- OMFS - Dr. Amit T. Suryawanshi.. Mandibular fractu...All Good Things
Dentist in pune. (BDS. MDS) - Dr. Amit T. Suryawanshi. Seminar-Canine Impaction.
Email ID- amitsuryawanshi999@gmail.com
Contact -Ph no.-9405622455
Subscribe our channel on youtube - https://www.youtube.com/channel/UC_gylEXTrjmEbbOTSXjuZ4Q/videos?view_as=public
Follow us on slideshare
Medical Technology Tackles New Health Care Demand - Research Report - March 2...pchutichetpong
M Capital Group (“MCG”) predicts that with, against, despite, and even without the global pandemic, the medical technology (MedTech) industry shows signs of continuous healthy growth, driven by smaller, faster, and cheaper devices, growing demand for home-based applications, technological innovation, strategic acquisitions, investments, and SPAC listings. MCG predicts that this should reflects itself in annual growth of over 6%, well beyond 2028.
According to Chris Mouchabhani, Managing Partner at M Capital Group, “Despite all economic scenarios that one may consider, beyond overall economic shocks, medical technology should remain one of the most promising and robust sectors over the short to medium term and well beyond 2028.”
There is a movement towards home-based care for the elderly, next generation scanning and MRI devices, wearable technology, artificial intelligence incorporation, and online connectivity. Experts also see a focus on predictive, preventive, personalized, participatory, and precision medicine, with rising levels of integration of home care and technological innovation.
The average cost of treatment has been rising across the board, creating additional financial burdens to governments, healthcare providers and insurance companies. According to MCG, cost-per-inpatient-stay in the United States alone rose on average annually by over 13% between 2014 to 2021, leading MedTech to focus research efforts on optimized medical equipment at lower price points, whilst emphasizing portability and ease of use. Namely, 46% of the 1,008 medical technology companies in the 2021 MedTech Innovator (“MTI”) database are focusing on prevention, wellness, detection, or diagnosis, signaling a clear push for preventive care to also tackle costs.
In addition, there has also been a lasting impact on consumer and medical demand for home care, supported by the pandemic. Lockdowns, closure of care facilities, and healthcare systems subjected to capacity pressure, accelerated demand away from traditional inpatient care. Now, outpatient care solutions are driving industry production, with nearly 70% of recent diagnostics start-up companies producing products in areas such as ambulatory clinics, at-home care, and self-administered diagnostics.
Medical Technology Tackles New Health Care Demand - Research Report - March 2...pchutichetpong
M Capital Group (“MCG”) predicts that with, against, despite, and even without the global pandemic, the medical technology (MedTech) industry shows signs of continuous healthy growth, driven by smaller, faster, and cheaper devices, growing demand for home-based applications, technological innovation, strategic acquisitions, investments, and SPAC listings. MCG predicts that this should reflects itself in annual growth of over 6%, well beyond 2028.
According to Chris Mouchabhani, Managing Partner at M Capital Group, “Despite all economic scenarios that one may consider, beyond overall economic shocks, medical technology should remain one of the most promising and robust sectors over the short to medium term and well beyond 2028.”
There is a movement towards home-based care for the elderly, next generation scanning and MRI devices, wearable technology, artificial intelligence incorporation, and online connectivity. Experts also see a focus on predictive, preventive, personalized, participatory, and precision medicine, with rising levels of integration of home care and technological innovation.
The average cost of treatment has been rising across the board, creating additional financial burdens to governments, healthcare providers and insurance companies. According to MCG, cost-per-inpatient-stay in the United States alone rose on average annually by over 13% between 2014 to 2021, leading MedTech to focus research efforts on optimized medical equipment at lower price points, whilst emphasizing portability and ease of use. Namely, 46% of the 1,008 medical technology companies in the 2021 MedTech Innovator (“MTI”) database are focusing on prevention, wellness, detection, or diagnosis, signaling a clear push for preventive care to also tackle costs.
In addition, there has also been a lasting impact on consumer and medical demand for home care, supported by the pandemic. Lockdowns, closure of care facilities, and healthcare systems subjected to capacity pressure, accelerated demand away from traditional inpatient care. Now, outpatient care solutions are driving industry production, with nearly 70% of recent diagnostics start-up companies producing products in areas such as ambulatory clinics, at-home care, and self-administered diagnostics.
For those battling kidney disease and exploring treatment options, understanding when to consider a kidney transplant is crucial. This guide aims to provide valuable insights into the circumstances under which a kidney transplant at the renowned Hiranandani Hospital may be the most appropriate course of action. By addressing the key indicators and factors involved, we hope to empower patients and their families to make informed decisions about their kidney care journey.
This document is designed as an introductory to medical students,nursing students,midwives or other healthcare trainees to improve their understanding about how health system in Sri Lanka cares children health.
CHAPTER 1 SEMESTER V - ROLE OF PEADIATRIC NURSE.pdfSachin Sharma
Pediatric nurses play a vital role in the health and well-being of children. Their responsibilities are wide-ranging, and their objectives can be categorized into several key areas:
1. Direct Patient Care:
Objective: Provide comprehensive and compassionate care to infants, children, and adolescents in various healthcare settings (hospitals, clinics, etc.).
This includes tasks like:
Monitoring vital signs and physical condition.
Administering medications and treatments.
Performing procedures as directed by doctors.
Assisting with daily living activities (bathing, feeding).
Providing emotional support and pain management.
2. Health Promotion and Education:
Objective: Promote healthy behaviors and educate children, families, and communities about preventive healthcare.
This includes tasks like:
Administering vaccinations.
Providing education on nutrition, hygiene, and development.
Offering breastfeeding and childbirth support.
Counseling families on safety and injury prevention.
3. Collaboration and Advocacy:
Objective: Collaborate effectively with doctors, social workers, therapists, and other healthcare professionals to ensure coordinated care for children.
Objective: Advocate for the rights and best interests of their patients, especially when children cannot speak for themselves.
This includes tasks like:
Communicating effectively with healthcare teams.
Identifying and addressing potential risks to child welfare.
Educating families about their child's condition and treatment options.
4. Professional Development and Research:
Objective: Stay up-to-date on the latest advancements in pediatric healthcare through continuing education and research.
Objective: Contribute to improving the quality of care for children by participating in research initiatives.
This includes tasks like:
Attending workshops and conferences on pediatric nursing.
Participating in clinical trials related to child health.
Implementing evidence-based practices into their daily routines.
By fulfilling these objectives, pediatric nurses play a crucial role in ensuring the optimal health and well-being of children throughout all stages of their development.
Health Education on prevention of hypertensionRadhika kulvi
Hypertension is a chronic condition of concern due to its role in the causation of coronary heart diseases. Hypertension is a worldwide epidemic and important risk factor for coronary artery disease, stroke and renal diseases. Blood pressure is the force exerted by the blood against the walls of the blood vessels and is sufficient to maintain tissue perfusion during activity and rest. Hypertension is sustained elevation of BP. In adults, HTN exists when systolic blood pressure is equal to or greater than 140mmHg or diastolic BP is equal to or greater than 90mmHg. The
The dimensions of healthcare quality refer to various attributes or aspects that define the standard of healthcare services. These dimensions are used to evaluate, measure, and improve the quality of care provided to patients. A comprehensive understanding of these dimensions ensures that healthcare systems can address various aspects of patient care effectively and holistically. Dimensions of Healthcare Quality and Performance of care include the following; Appropriateness, Availability, Competence, Continuity, Effectiveness, Efficiency, Efficacy, Prevention, Respect and Care, Safety as well as Timeliness.
Global launch of the Healthy Ageing and Prevention Index 2nd wave – alongside...ILC- UK
The Healthy Ageing and Prevention Index is an online tool created by ILC that ranks countries on six metrics including, life span, health span, work span, income, environmental performance, and happiness. The Index helps us understand how well countries have adapted to longevity and inform decision makers on what must be done to maximise the economic benefits that comes with living well for longer.
Alongside the 77th World Health Assembly in Geneva on 28 May 2024, we launched the second version of our Index, allowing us to track progress and give new insights into what needs to be done to keep populations healthier for longer.
The speakers included:
Professor Orazio Schillaci, Minister of Health, Italy
Dr Hans Groth, Chairman of the Board, World Demographic & Ageing Forum
Professor Ilona Kickbusch, Founder and Chair, Global Health Centre, Geneva Graduate Institute and co-chair, World Health Summit Council
Dr Natasha Azzopardi Muscat, Director, Country Health Policies and Systems Division, World Health Organisation EURO
Dr Marta Lomazzi, Executive Manager, World Federation of Public Health Associations
Dr Shyam Bishen, Head, Centre for Health and Healthcare and Member of the Executive Committee, World Economic Forum
Dr Karin Tegmark Wisell, Director General, Public Health Agency of Sweden
ICH Guidelines for Pharmacovigilance.pdfNEHA GUPTA
The "ICH Guidelines for Pharmacovigilance" PDF provides a comprehensive overview of the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH) guidelines related to pharmacovigilance. These guidelines aim to ensure that drugs are safe and effective for patients by monitoring and assessing adverse effects, ensuring proper reporting systems, and improving risk management practices. The document is essential for professionals in the pharmaceutical industry, regulatory authorities, and healthcare providers, offering detailed procedures and standards for pharmacovigilance activities to enhance drug safety and protect public health.
Empowering ACOs: Leveraging Quality Management Tools for MIPS and BeyondHealth Catalyst
Join us as we delve into the crucial realm of quality reporting for MSSP (Medicare Shared Savings Program) Accountable Care Organizations (ACOs).
In this session, we will explore how a robust quality management solution can empower your organization to meet regulatory requirements and improve processes for MIPS reporting and internal quality programs. Learn how our MeasureAble application enables compliance and fosters continuous improvement.
TOP AND BEST GLUTE BUILDER A 606 | Fitking FitnessFitking Fitness
"Feature:
• Intelligent Ergonomically Design Glute Builder Is A Must Have For Those Looking To Target Their Gluteal Muscles And Hamstrings With Precision.
• The Ability To Adjust The Starting Position, This Machine Allows For A More Targeted Workout That Is Tailored To Your Specific Needs.
• Spacious And Supportive Cushioned Seat Provide Added Comfort And Stability During Your Workout."
Get more information visit on:- www.fitking.in
Our mail I.D:-care@fitking.in, fitking.in@gmail.com
Call us at :- 9958880790, 9870336406, 8800695917
CHAPTER 1 SEMESTER V PREVENTIVE-PEDIATRICS.pdfSachin Sharma
This content provides an overview of preventive pediatrics. It defines preventive pediatrics as preventing disease and promoting children's physical, mental, and social well-being to achieve positive health. It discusses antenatal, postnatal, and social preventive pediatrics. It also covers various child health programs like immunization, breastfeeding, ICDS, and the roles of organizations like WHO, UNICEF, and nurses in preventive pediatrics.
3. Definition
• A fracture is a disruption in the continuity of a
bone stressed beyond its elastic modulus, with
the formation of two or more fragments.
4. I. Location of problem to be treated.
II. Diagnosis & treatment plan
III. Documentation
IV. Assessment of treatment
V. Epidemiological studies
5. • Direct or indirect
• Complete or incomplete
• Mechn- bending, torsion, shear, contrecoup. avulsion and
burst type
• Site
• Displacement
• Number-single ,multiple or comminuted
• Integument- closed or open
• Shape- transverse ,oblique butterfly,
• oblique surface fracture
10. 1. Number of fracture /fragments ( F)
2. location of fracture ( L)
3. Status of occlusion (O)
4. Soft tissue involvement (S)
5. Associated injuries (A)
11. • F0- Incomplete fracture
• F1- Single fracture
• F2-Multiple fracture
• F3-Comminuted fracture
• F4-Fracture with a bony defect
18. • S0-closed
• S1-open intraorally
• S2-open extraorally
• S3-open intra and extraorally
• S4-soft tissue defect
19. • A0-None
• A1-Fracture or loss of tooth
• A2-Nasal bone
• A3-Zygoma
• A4-Le Fort I
• A5-Le Fort II
• A6-Le Fort III
20.
21. • Three stages-
Immediate assessment and treatment of any condt
constituting a threat to life
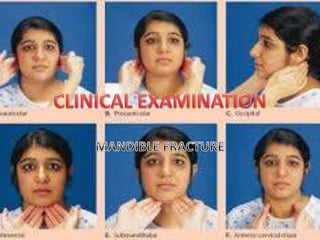
General clinical examination
Local examination
22. • Mf injuries may associated with body injuries may constitute threat to life
than facial trauma
• Rapid survey & Assessment
A-Airway
B-Breathing & Ventilation
C-Circulation & Hemorrhage control
D-Disability-Neurological assessment
E-exposure to external environment
27. • Recognition
Central pulse –Femoral /carotid
Skin colour-pink-ashen grey-white
Level of consciousness-confusion-aggression-drowsiness-
coma
Pulse- 120/min ( very thready)
Respiratory rate-20/min- Tachypnea
Weakness-due to hypoxia ,acidosis
Urinary out put- >30 ml/hr- 0-10 ml/hr
28. • Fluid replacement- Crystalloids. Colloids, Blood
• Local-( Maxillofacial aspect)
Pressure pack
Ligation of Vessel
Direct dental wiring at fracture region
29.
30.
31. • Careful clinical examination and no operative intervention
without rule out additional more serious injuries
• If cerebral hemorrhage , loss of consciousness
• Additional injuries required urgent treatment than MF injuries
• In polytrauma pt treated concurrently
• Major injuries- careful inspection/palpation reveal their
presence –treated accordingly
32. • If fracture mandible pt in
shocked, very unusual,
• Some more serious
condition other than
fracture mandible should be
suspected and treated
• first
33.
34. • Preparation for examination
• Face-gently cleaned with warm water
• Remove road dirt etc-evaluation of soft tissue injury
• Mouth-loose ,broken teeth,or dentures,any congealed blood
removed with swab in nontooth forcep
• If denture-full/ pieces reassemble piece so portion should be
missing-possibly displaced down into throat
• Complete extra & intra oral cleaning-assess full extent of injury
35. • During cleaning cranium and cervical spine should be carefully
inspected and palpated for sign of injury
36. Extravsation of blood from
injured bone resulted swelling
of face-more swelling increase
capillary permeability and
edema
Swelling+ecchymosis-fracture
Facial deformity-fracture &
displaced fragment
Open hang mouth-B/L condylar
#
37.
38. • Conscious pt- support his jaw with own hand
• Compound fracture- blood stained saliva may dribbled out from
corner of mouth
• Palpation-begin from bilateral condylar region-
downwards posterior along lower border of mandible.
• Any bone tenderness- pathognomic of fracture
• Deformity /bony cerpitus present
• Anesthesia/ paresthesia- injury to IAN- reduced or absent sensation
On one or both side of the lower lip
39.
40.
41.
42. Intra Oral Examination
Clean oral cavity-lukewarm mouth
wash/ cleaned with moistened
swab
Congealed blood,fragments of
tooth,alveolus,denture removed
with forcep/ suction tip
Buccal & Libgual sulci-
ecchymossis,submucosal
extravastion of blood-#
43. • Any lingual mucosa hematoma-#
• Bec lingual mucosa directly overlied periosteum of mandible
• Linear hematoma in third molar reg-indi fracture
44.
45. Edentoulus/ alv ridge
Step in occlusion,laceration in
overlying mucosa
Tooth-
luxation/subluxation,crown
fracture/dentine/pulp exposed ?
Any loose filling,fine crack/split
tooth
Missing-tooth,f illing, crown,
denture, portion of tooth-
CHEST X-RAYS
46. • Fracture site- mobility placing
finger and thumb on each side
and using pressure to elicit
mobility
• Any pain in jaw movement
recorded.
• Flat of both hands placed over
two angles of mandible and
gentle pressure exerted-if pain
• If crack fracture is present
48. • Direction and intensity of the traumatic force.
• Site of fracture
• Direction of fracture line
• Muscle pull exerted on the fractured fragments
• Presence or absence of tooth.
• Extent of soft tissue wounds
50. Injury
Pain- pain upon movement r remote from the site of injury
Abnormal mobility-abn mobility in dental arches r during jaw
movement.
Bleeding- active bleeding / hematoma or ecchymosis may
follow a fracture process.
Crepitus- Cracking, grating sound can be detected during
palpation of injury site.
51. Deformity-facial deformity depending upon degree and
direction of impact, also direction of fracture line and muscle
pull also.
Ecchymosis- and edma- seen extra orally and intraorally
depending upon impact and site of fracture.
Loss of function or interference with function-Mastication
problem, speech and difficulty in swallowing.
52. • Paresthesia/ hypoesthesia of lower lip- fracture between
mental foramen and ramus region
• Radiographic evidence-all suspected cases must be
radiographed. help as diagnostic aid and addition
confirmation also for medico legal documentation and as
evidence.
54. • Dento alveolar
• Condylar
• Coronoid Process
• Ramus
• Angle
• Body
• Symphysis & para symphysis
• Comminuted fracture
Anatomical
55. • Avulsion/subluxation or fracture of tooth in
association with fracture of alveolus.
• DA fracture alone
• DA plus mandibular fracture
56. • Laceration, full thickness wound of lower lip-imp low
teeth
• complete loss of soft tissue
• Bruising with embeded tooth portion/ foreign body
• Alv margin-laceration of gingiva, deformity of alveolus
• Degloving injury
57.
58. • Impaction of point of chin on some resilient surface-soft earth
• Jaw does not fracture but soft tissue rotated violently over
point of chin. horizontal tear at junction of attached & free
gingiva
59. • Tooth- lost, recent extn wound-knocked out
• Split/ Fracture- premolar & Molars- horizontal / vertical split
below the gingival margin-indirect trauma from opposing
dentition
• Crown- fracture, embedded into soft tissue, swallowed or
inhaled.
60. • If pulp/near pulp exp-immediate treatment
• Root- fracture, excessive mobile tooth, subluxated ?
• IOP Xrays
• Thermal sensitivity-unreliable to test injury to pulp
• Trauma/ force –disturb the function of nerve endings
61. • Isolated fracture
• With injury to tooth
• Gross comminution of Alveolus
• Alv fracture consists one or two fragments containing teeth
• Complete Alv Fr+ Teeth segment displaced into soft tissue of
the floor of mouth covered by mucosa.
•
62. • +-Difficult to differentiate alveolar fracture from symphysis
fracture-
• Unless palpate at lower border of mandible.
• During examn easy to reposition the alveolar fracture
fragment in position-better prognosis.
63. • Most common overall fracture ( 20 % )
• Easily missed fracture during examination
64. • Unilateral / Bilateral
• Intra capsular / Extra capsular( condylar Neck).
• Extra capsular type-with or without dislocation
65. • Inspection-
• Swelling over joint - +
• bleeding from ear( laceration of antr wall of EAM
• D/D-bleeding from middle ear +CSF otorrhoea- Petrus
temporal bone #
• Ecchymosis of skin below mastoid process-when hematoma
surrounding fractured condyle tracked down to EAM.
• D/D Battle Sign ( Base of Skull # )
• If mandible locked- when condyle impacted through glenoid
fossa
66. • If condyle medially dislocated-when edema subsided hollow
characteristic sign will be present
• Immediate post trauma-sign obscured by edema.
67. • Tenderness over condylar area
• EAM palpation –when condyle is dislocated from glenoid fossa.(standing
in front of pt both little can be hooked into each EAM ).
• Rarely hemorrhage from condylar region track across the base of skull-
exert pressure on mand. Divin. Of Vth N at F.Ovale-paresthesia of lower lip
• D/D-Fracture of Body / Angle region of mandible rule out
68. Condyle dislocated resulted
ramus height shortening-
Molar gagging of the occlusion.
Deviation of mandible towards fracture side.
Painful movements- Lateral excursion to
opposite side
-Protrusive movement .
69. • Extra orally- same sign & symptoms bilaterally
• Mandibular movement restricted.
• Intra orally-
• In intra capsular fracture bilaterally- if any ramal shortening but normal
occlusion.
• Extracapsular #- b/L condylar dislocation- B/L ramus shortening
/overriding of fracture fragments- Antr open bite.
• Painful & limited opening movements.
• Painful & restricted protusion n lateral excursions
70.
71. Guard man fracture- B/L condylar fracture with Symphy or
Parasymphysis fracture
72. • Rare fracture
• Result from reflux contracture of powerful antr fibres of
temporalis muscle.
• Direct trauma to ramus- # coronoid process
• Tip #-pulled upwards into infratemporal space ( Temp M )
• Sometime- surgery of cyst r large tumor of the ramus.
• Palp-tenderness over antr part of ramus, tell-tele hematoma
• Painful, limited protrusive movement.
73. • Not common- two types
• Single fracture- Low condylar fracture-both condyle &
coronoid process on upper fragment.
• Comminuted Fracture- direct violence from gun shot/missile
injury- fragments splinted between masseter muscle and
medial pterygoid muscles with little or no displacement.
74. Swelling & ecchymosis extra & intraorally.
Tenderness over the ramus .
Severe trismus present ?
75. • Inspection-
Swelling
Facial deformity
I/O step deformity behind last molar
Presence of hematoma Buccal r lingual side or both adjacent
to fracture.
Anesthesia or paresthesia of the lower lip.
Occlusion-deranged.
76.
77.
78. • Palpation-
Tenderness present at angle region
Movement /crepitus at fracture site ( if ramus steadied
between finger and thumb and body of mandible
moved gently with the other hand) .
Step may palpated.
Painful restricted jaw movements.
79. • Swelling
• Tenderness
• Displaced fractured fragment, causes derangement of occlusion
• Premature contacts in distal fragment (displacing action of muscles
attached to Ramus)
• Occlusion Derangement.
• Gingival tear due to its firm attachment -displaced fragments
80. • If gross displacement can
cause Intra oral
hemorrhage-IAA torned ?
• Molar & Premolar tooth-
split longitudinally /
vertically- considerable
discomfort
82. • Commonly associated with one /both condyle.
• Presence of bony tenderness & lingual hematoma important
sign-
• Bec antr mandible thickness between often ensure fine
cracks with little displacement.
• May be missed if occlusion is undisturbed locally.
•
83. Bony tenderness and small lingual hematoma may be only
physical sign present
Severe impact( direct violence-oblique fracture-displaced
fragments. Which allows over riding of the fragments with
lingual inversion of the occlusion on each side.
Always associated soft tissue injury of chin and lower lip
84. • Detachment of genioglossus M – may contribute loss of
tongue control.
• Airway obstruction.
• If Pt Conscious- voluntarily control of tongue
prevent obstruction.
• If unconscious- stay suture of tongue/airway
to prevent tongue fall.
• No paresthesia of skin of mental region unless
mental nerve is involved.
Editor's Notes
mobility placing finger and thumb on each side and using pressure to elicit mobility