Downloaded 764 times
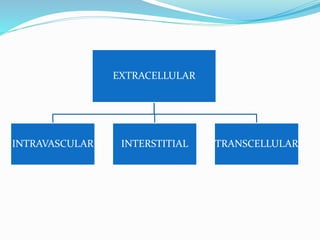
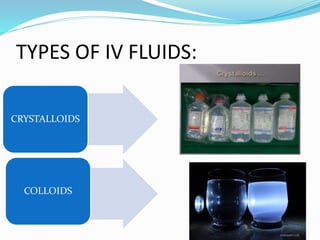
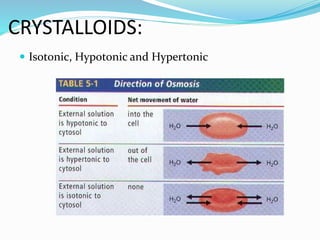
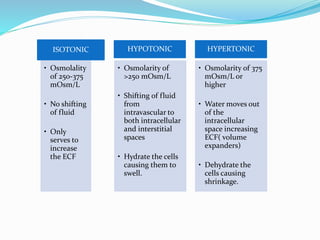
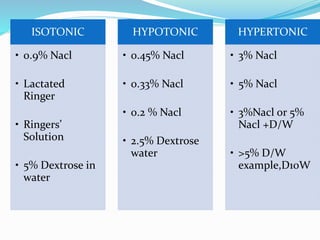
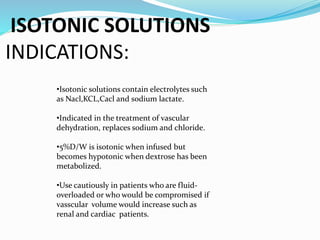
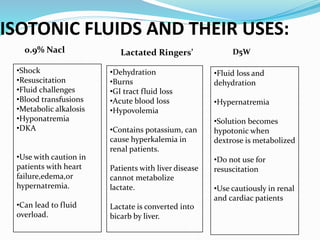
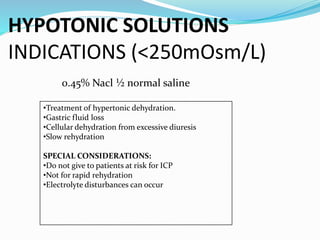
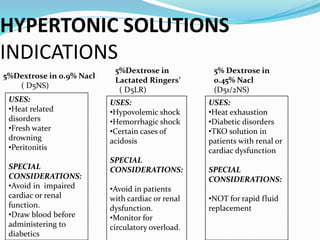
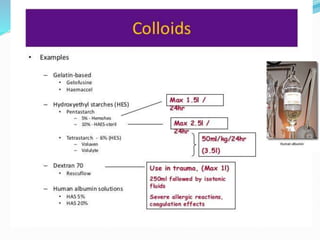



This document discusses intravenous (IV) therapy, including the types of IV fluids used and their indications. It describes crystalloid fluids as isotonic, hypotonic, or hypertonic depending on their osmolarity and effect on fluid shifts. Isotonic fluids like 0.9% NaCl are used for dehydration while hypotonic fluids help with hypertonic dehydration. Hypertonic fluids shift fluid out of cells. Colloid fluids also shift fluid out of cells and are used for shock. The document stresses avoiding too much or too little IV fluid and cautions about fluid overload, electrolyte disturbances, and rapid changes in sodium levels that can harm patients.



































































