Downloaded 83 times


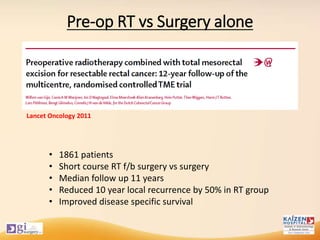


1. Neoadjuvant chemoradiotherapy (CTRT) followed by total mesorectal excision (TME) surgery has become the standard of care for locally advanced rectal cancer based on improved local control and survival outcomes compared to surgery or radiotherapy (RT) alone. 2. The addition of chemotherapy to neoadjuvant RT improves pathological complete response rates and local control compared to RT alone, though it also increases toxicity. 3. For patients who achieve a clinical complete response after neoadjuvant CTRT, a non-operative "watch and wait" approach may be considered given comparable oncologic outcomes when salvage surgery is performed for recurrences.























































































