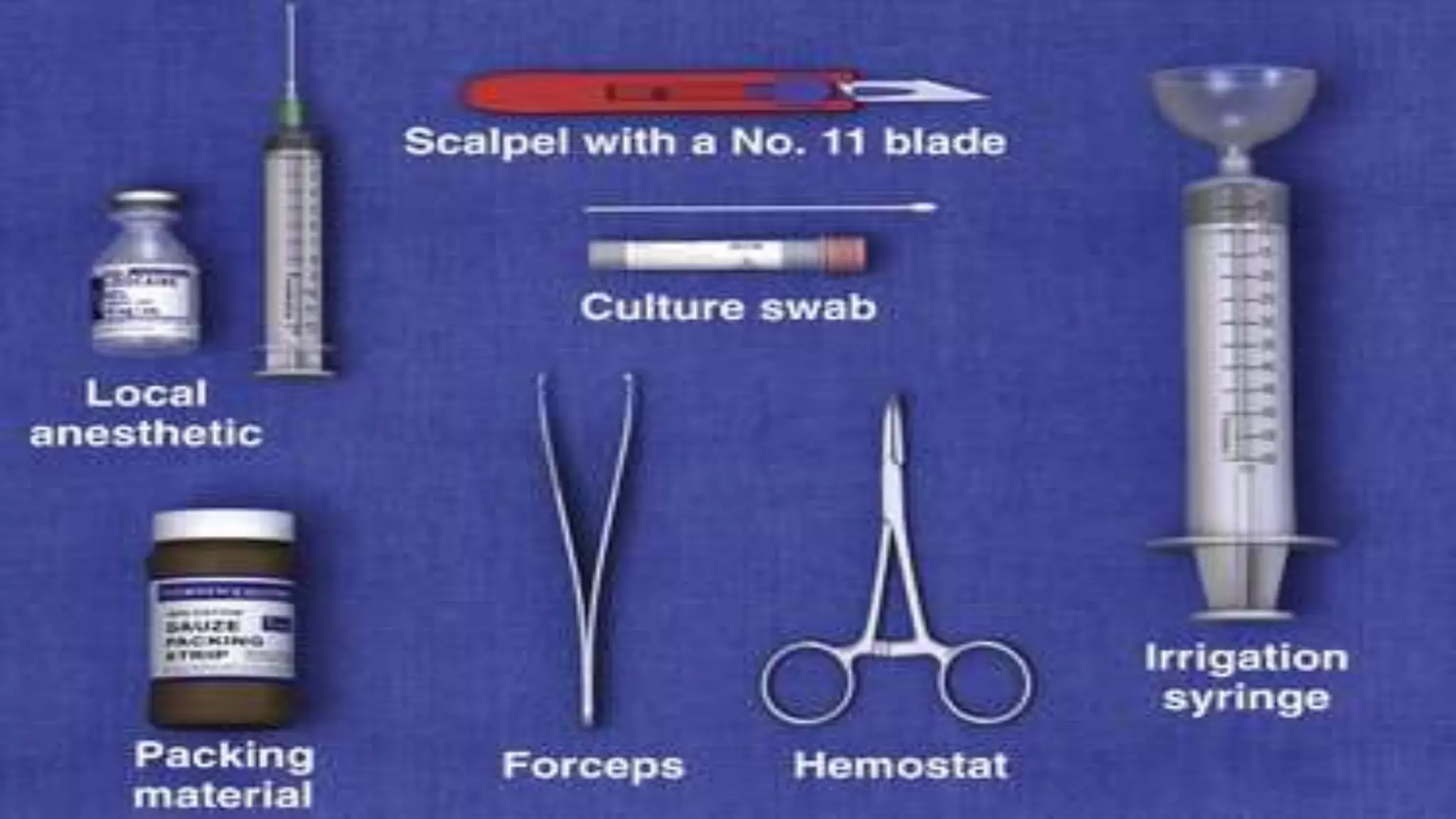
This document describes the procedure for incision and drainage of an abscess. It outlines the objectives of relieving pressure and pain and draining pus/debris. Abscesses larger than 5mm in accessible areas are indications for the procedure. The incision should be made in the most dependent part of the swelling, parallel to skin lines. The abscess cavity is opened, locules are broken up, and the cavity is irrigated and may be packed or drained. Complications can include insufficient pain relief or progression to worsening cellulitis.