Water Seal Drainage
•
10 likes•5,080 views

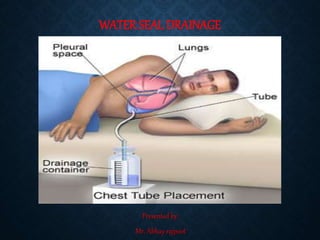
Chest drains also known as under water sealed drains (UWSD) are inserted to allow draining of the pleural spaces of air, blood or fluid, allowing expansion of the lungs.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Water Seal Drainage
Similar to Water Seal Drainage (20)
More from Abhay Rajpoot
More from Abhay Rajpoot (20)
Recently uploaded
Recently uploaded (20)
Water Seal Drainage
- 1. WATER SEAL DRAINAGE Presented by: Mr. Abhay rajpoot
- 2. DEFINITION: Nasogastric tube: A tube that is passed through the nose and down through the nasopharynx and esophagus into the stomach. It can be used to remove the contents of the stomach, including air, to decompress the stomach, or to remove small solid objects and fluid, such as poison, from the stomach.
- 4. TYPES OF TUBES: Short tubes: passed through the nose into the stomach: range in size from 14 to 18 Fr, single lumen made of plastic or rubber with holes near the tip. Medium Tubes: tubes are passed through the nose to the duodenum and the jejunum. Long tubes: passed through the nose, through the esophagus and stomach into the intestines. Used for decompression of the intestines.
- 5. INDICATIONS FOR GI INTUBATION
- 6. INSERTION OF AN NG TUBE Assessment: − Who needs an NG: Surgical clients Ventilated client Neuromuscular impairment. Clients who are unable to maintain adequate oral intake to meet metabolic demands.
- 7. CONTI….. − Assess patency of nares: Assess client’s medical history: Nosebleeds Nasal surgery Deviated septum Anticoagulation therapy – Assess client’s gag reflex. – Assess client’s mental status. – Assess bowel sounds-
- 8. PLANNING: Gather equipment: 14 0r 16 Fr NG tube Lubricating jelly Flashlight Emesis basin Catheter tipped syringe 50 ML syringe Bowl with water Stethoscope
- 9. CONTI…… • Explain procedure to client • Position the client in a sitting or high fowlers position. • Examine feeding tube for flaws. • Determine the length of tube to be inserted. • Measure distance from the tip of the nose to the earlobe and to the xyphoid process of the sternum. • Prepare NG tube for insertion.
- 10. RISKS OF NASOGASTRIC INSERTION NG tube feeding can also potentially cause: -Abdominal cramping -Abdominal swelling -Diarrhea -Nausea -Vomiting -Regurgitation of food or medicine
- 11. MEASUREMENT:
- 12. IMPLEMENTATION−
- 14. CONTI….Emphasize the need to mouth breathe and swallow during the procedure. Swallowing facilitates the passage of the tube through the oropharnyx. Advance tube each time client swallows until desired length has been reached. Do not force tube. Check placement of the tube. − X-ray confirmation − Aspiration
- 15. NG TUBE INSERTION: NasogastricTube Position:
- 16. EVALUATION: Observe client to determine response to procedure. ALERTS!!! Persistent gagging –Prolonged intubation and stimulation of the gag reflex can result in vomiting and aspiration −Coughing may indicate presence of tube in the airway. Note location of external site marking on the tube Documentation
- 17. RESPONSIBILITIES: Identify signs and symptoms of inadvertent respiratory migration. Identify conditions that increase the risk for spontaneous tube dislocation from the intended position (retching, vomiting, nasotracheal suctioning, severe coughing) Enteral Nutrition.
- 18. BIBLIOGRAPHY: • https://www.healthline.com/health/nasogastric-intubation-and- feeding#purpose • https://www.wikihow.com/Insert-a-Nasogastric-(NG)-Tube • https://www.wikihow.com/Insert-a-Nasogastric-(NG)-Tube • https://en.wikipedia.org/wiki/Nasogastric_intubation • https://www.nursingtimes.net/clinical- archive/gastroenterology/nasogastric-tubes-1-insertion-technique- and-confirming-position/5000781.article