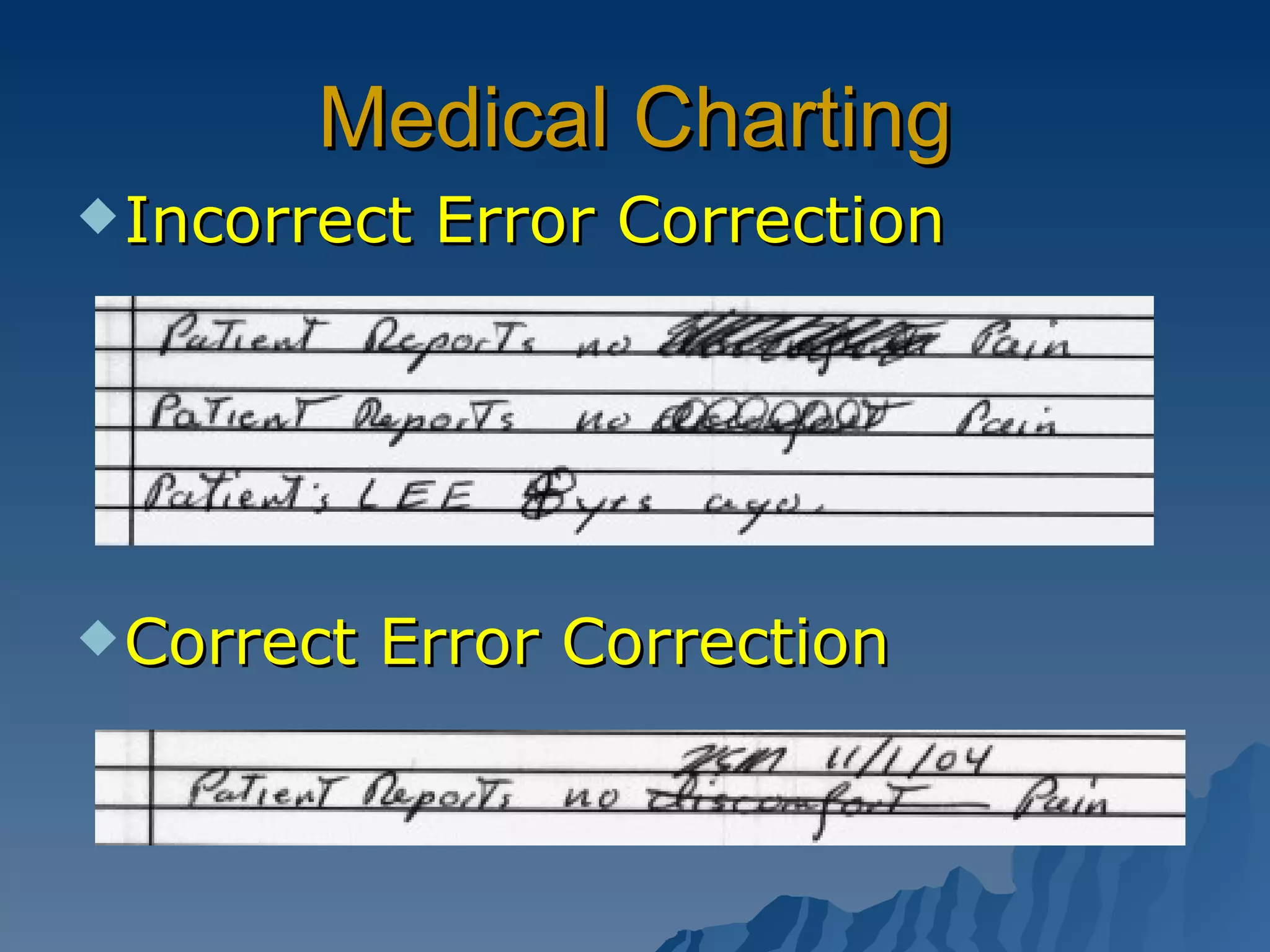
The document discusses medical documentation, charting, terminology, and related guidelines. It covers the purposes of medical records including patient care, continuity of care, reimbursement, and legal defense. It provides guidelines for documentation, terminology, abbreviations, and maintaining confidentiality. Key elements that must be included in medical records are also outlined.