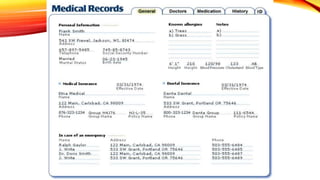
The document discusses medical records, including their purpose and components. Medical records serve both clinical and non-clinical purposes, providing a record of a patient's medical history and care. They support continuity of care and include information such as diagnoses, treatments, test results, and notes from healthcare professionals. Key components of medical records include personal identification information, diagnostic information, physical exam findings, and documentation of treatment plans and outcomes. Accuracy, completeness, timeliness and confidentiality are important principles for proper medical record documentation.