Downloaded 780 times

This document discusses hallux valgus, a deformity of the great toe. It begins by describing the anatomy and pathophysiology, noting that hallux valgus has no single cause but can be due to conditions like flat feet or footwear. Clinical presentation includes bunion pain that worsens with footwear. Treatment involves modifying footwear, splinting, and surgery if conservative measures fail. Surgical options correct soft tissues like tendons and ligaments as well as bony procedures like osteotomies of the toe bone or metatarsal. Complications of surgery include recurrence of the deformity or issues like nerve damage.
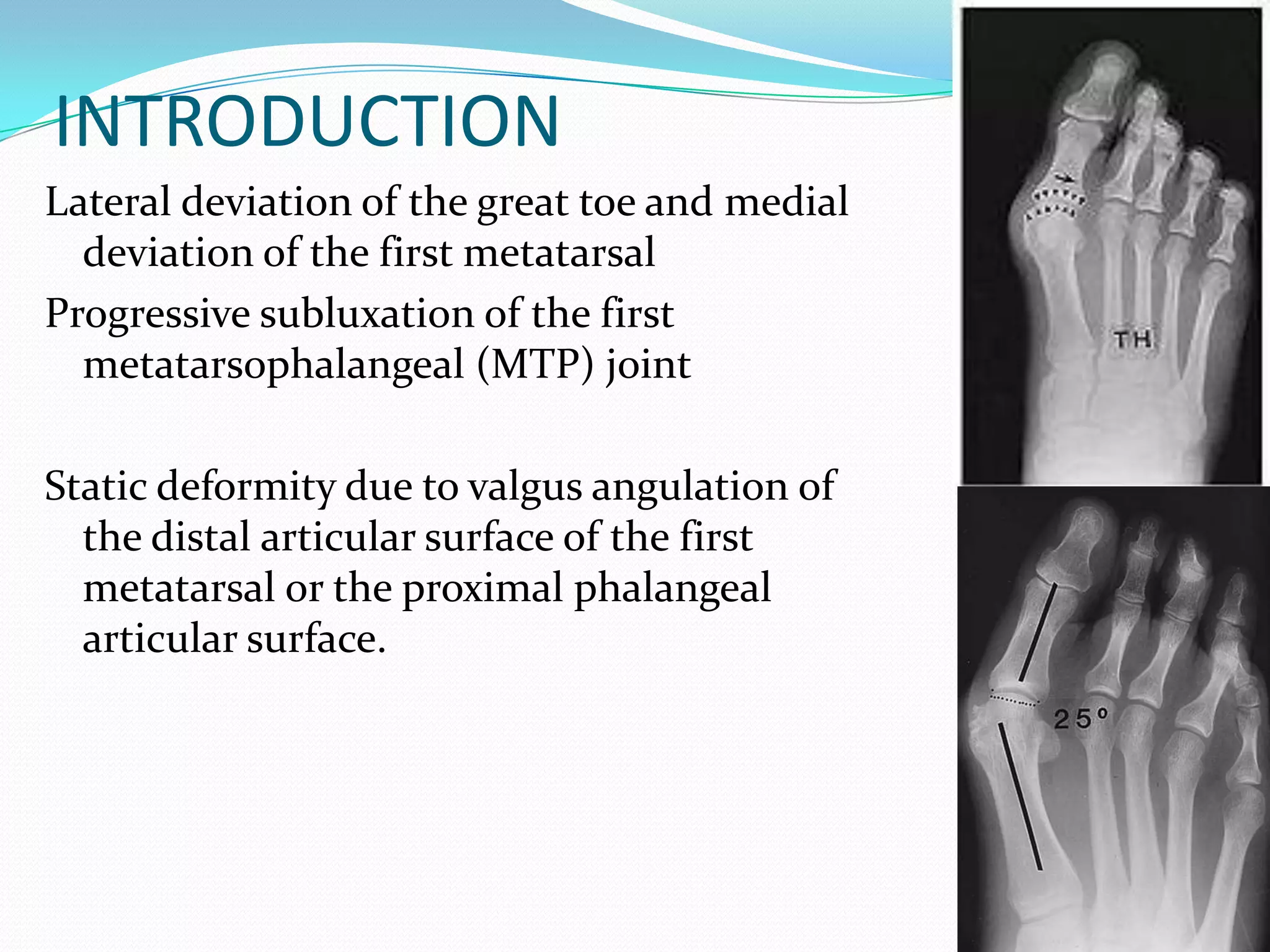
Presentation by Dr. Dhananjaya Sabat, detailing hallux valgus as a lateral deviation of the great toe and its static deformity.
Hallux valgus lacks a single cause; associated factors include metatarsus primus varus, footwear, age, gender, and rheumatoid arthritis.
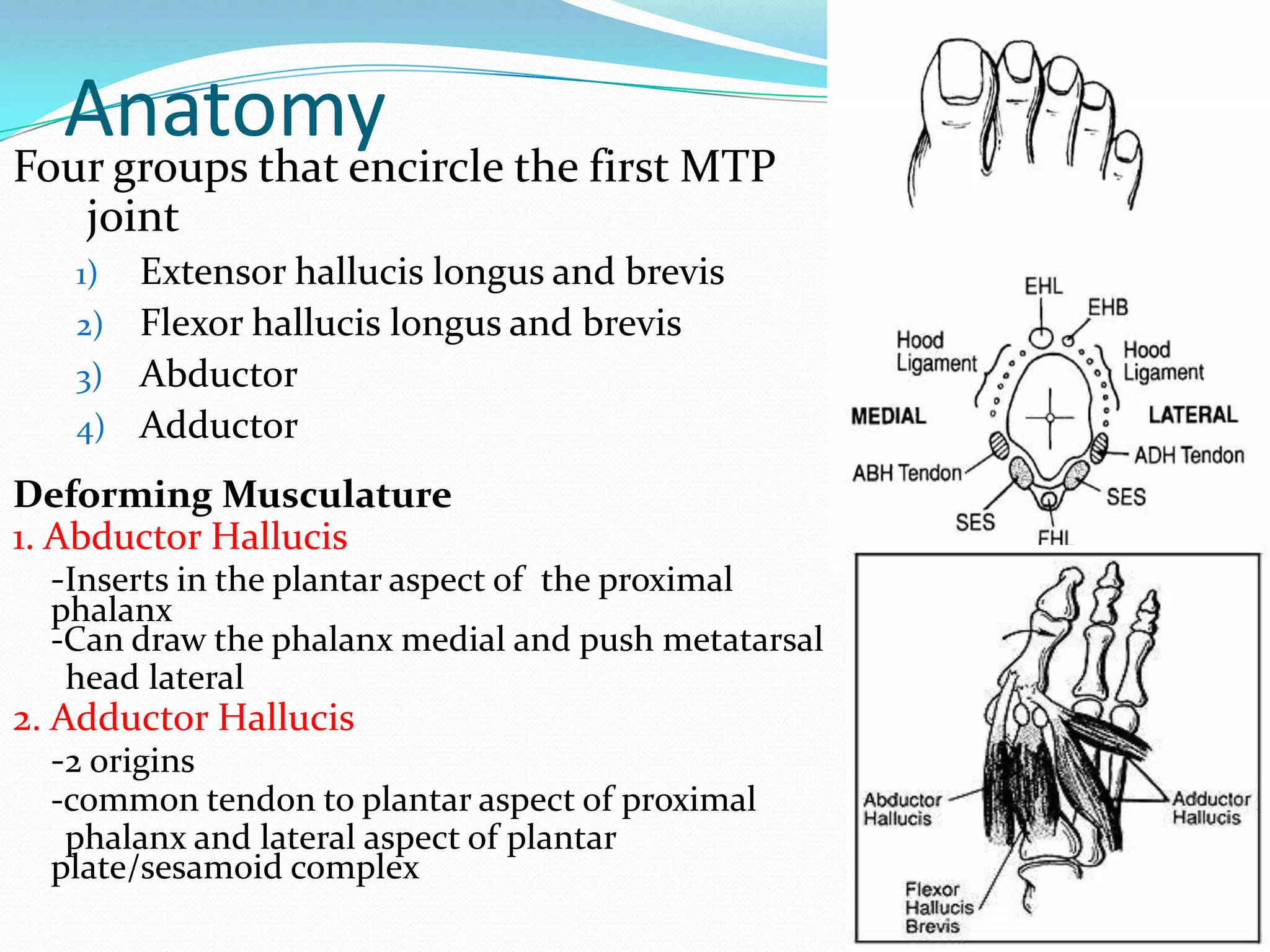
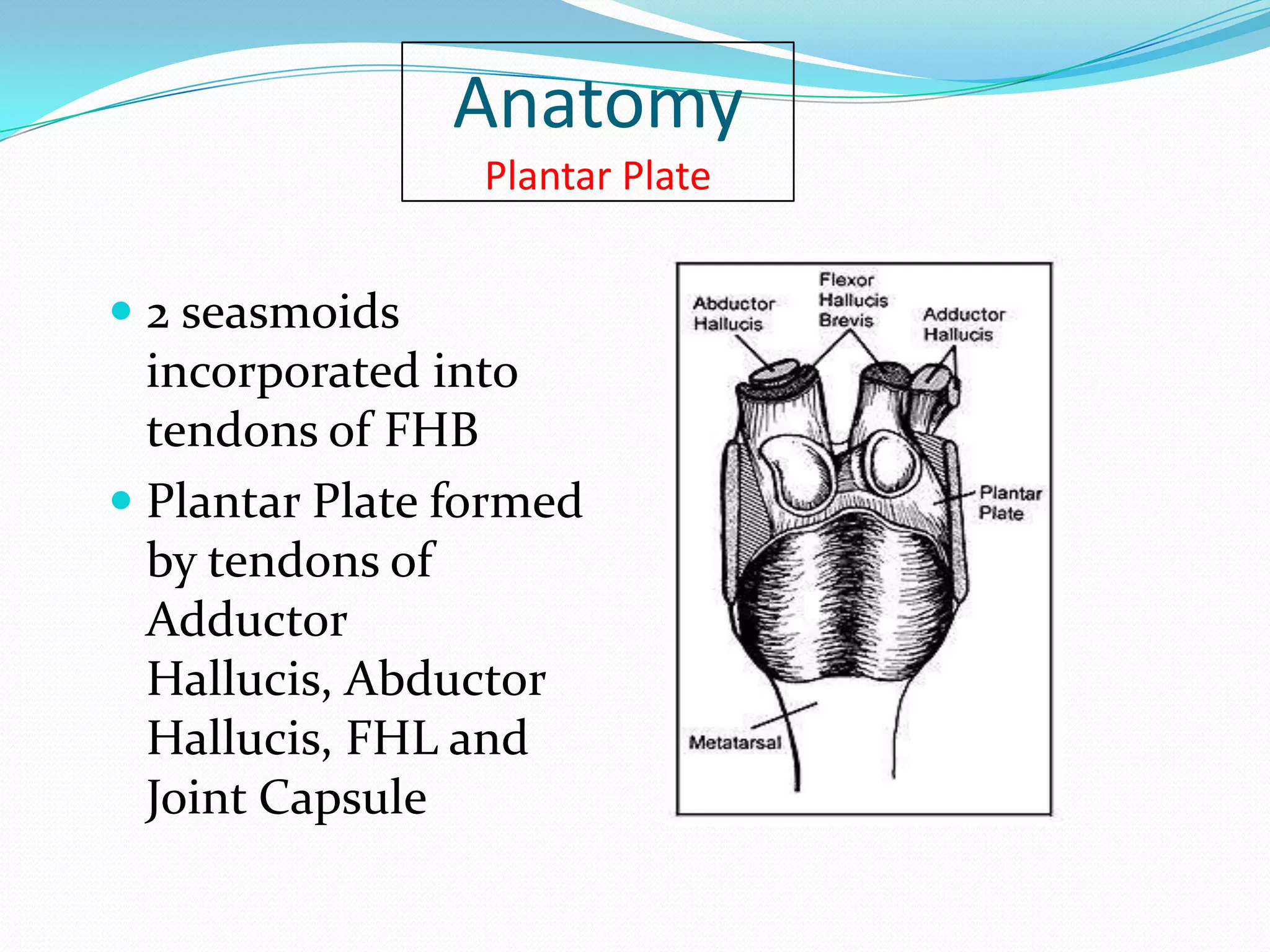
Anatomical structures surrounding the first MTP joint including muscles that contribute to the deformity, and the plantar plate.
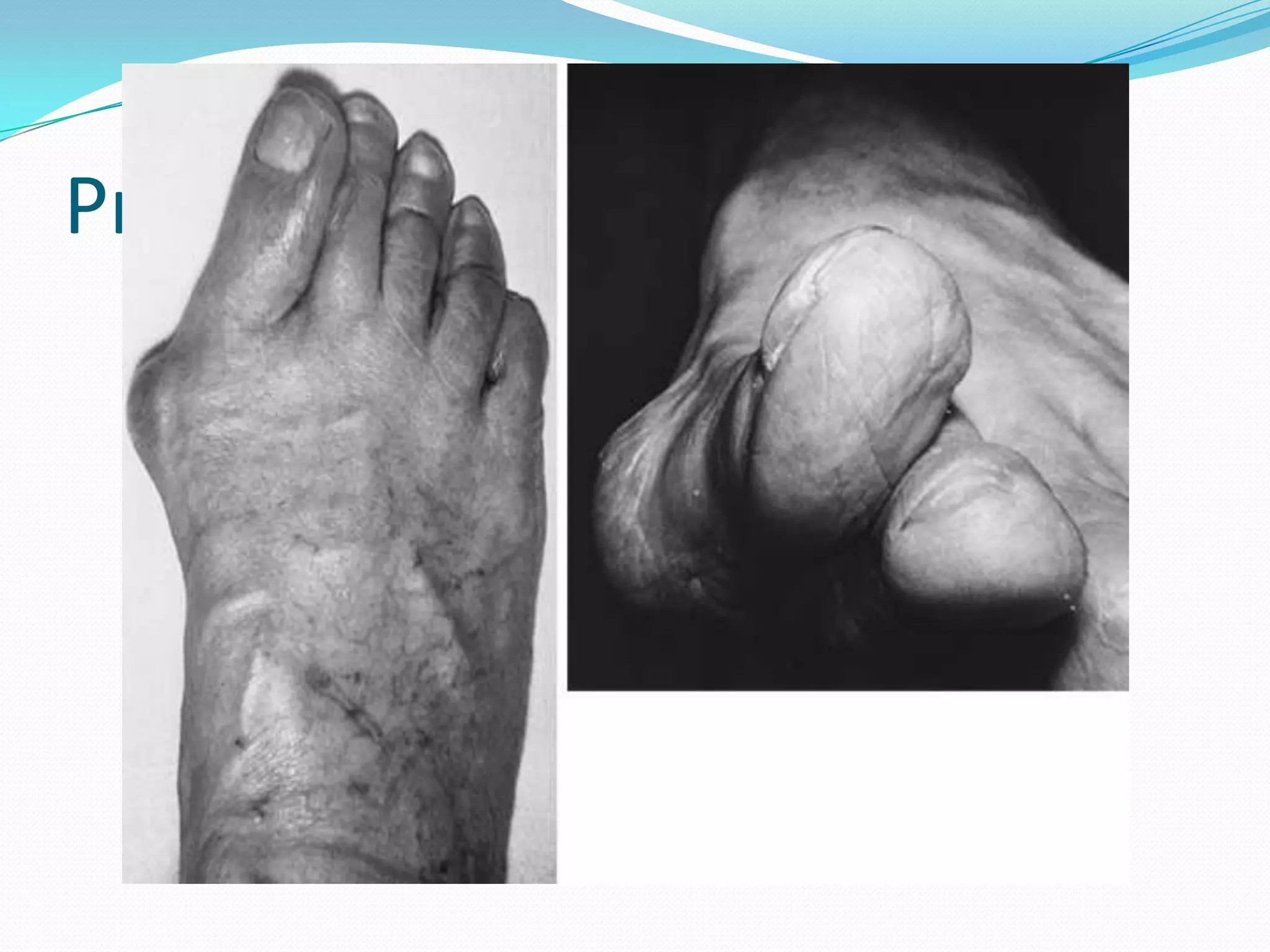
Bunion characterized by pain, bursal inflammation, and skin breakdown due to pressure from footwear.
Physical assessment highlights include skin condition, 1st MTP motion, and evaluation for foot deformities like pes planus.
Weightbearing radiographs assess bone and joint deformities, evaluating the alignment and congruency of the MTP joint.
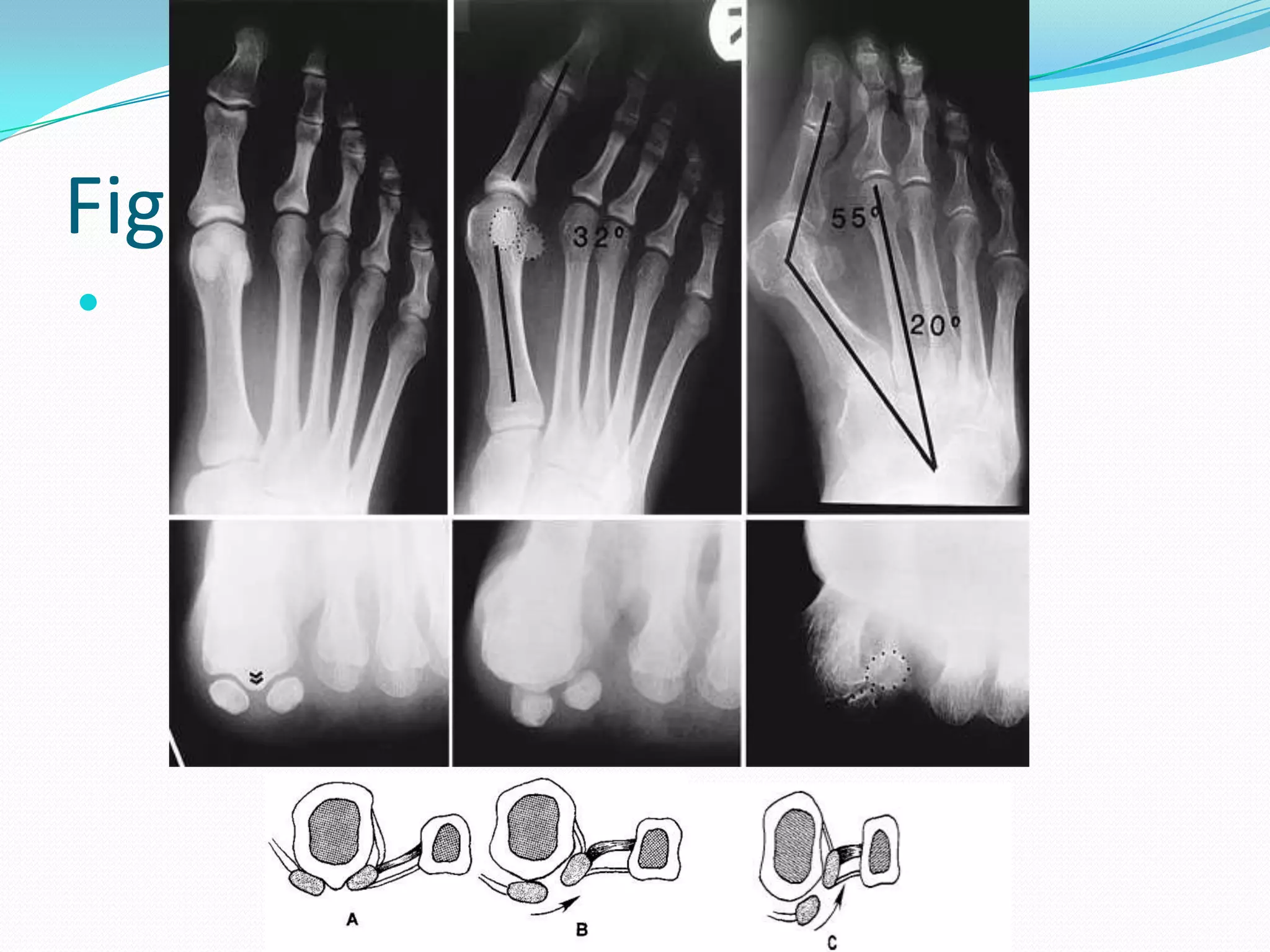
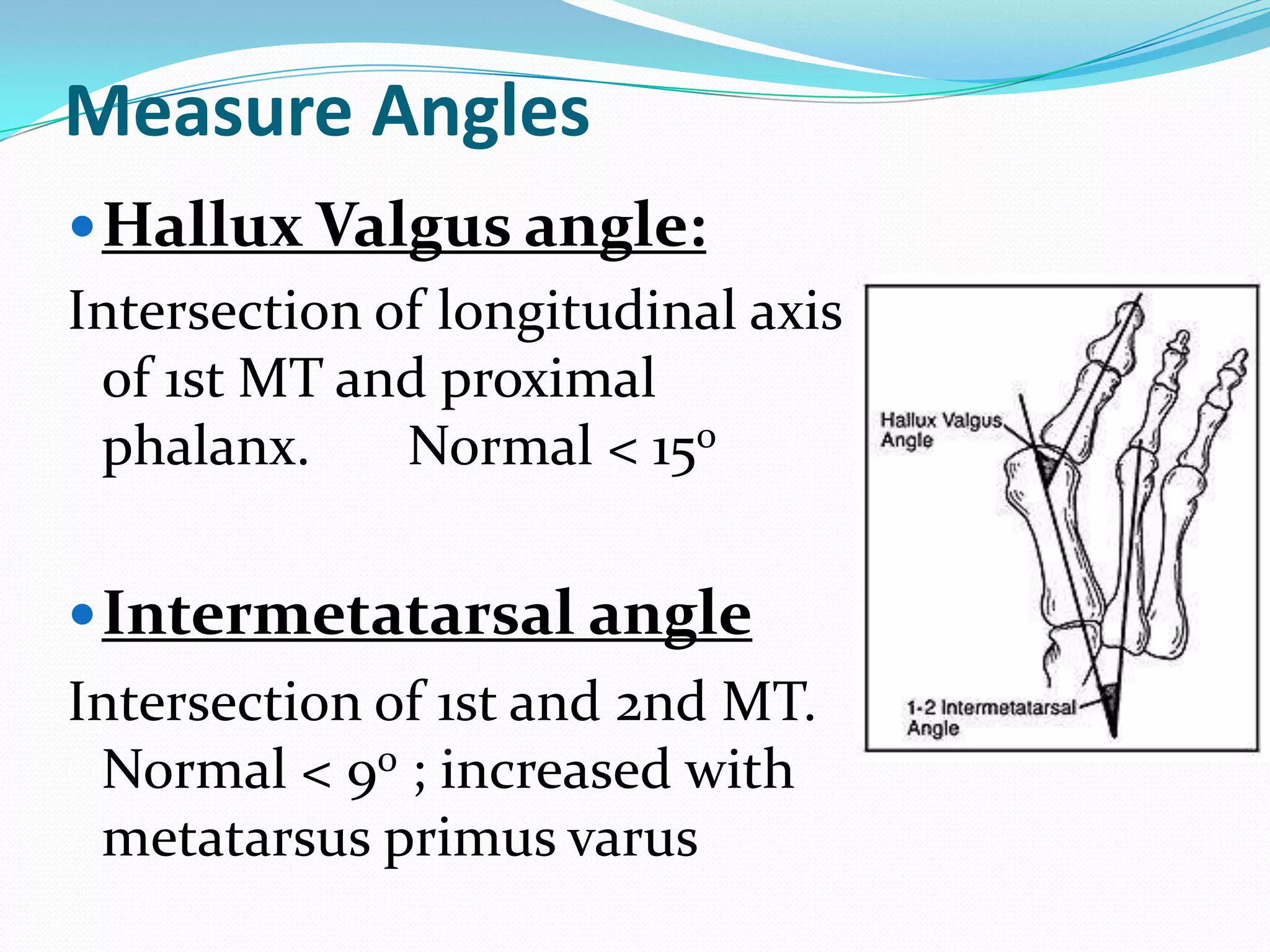
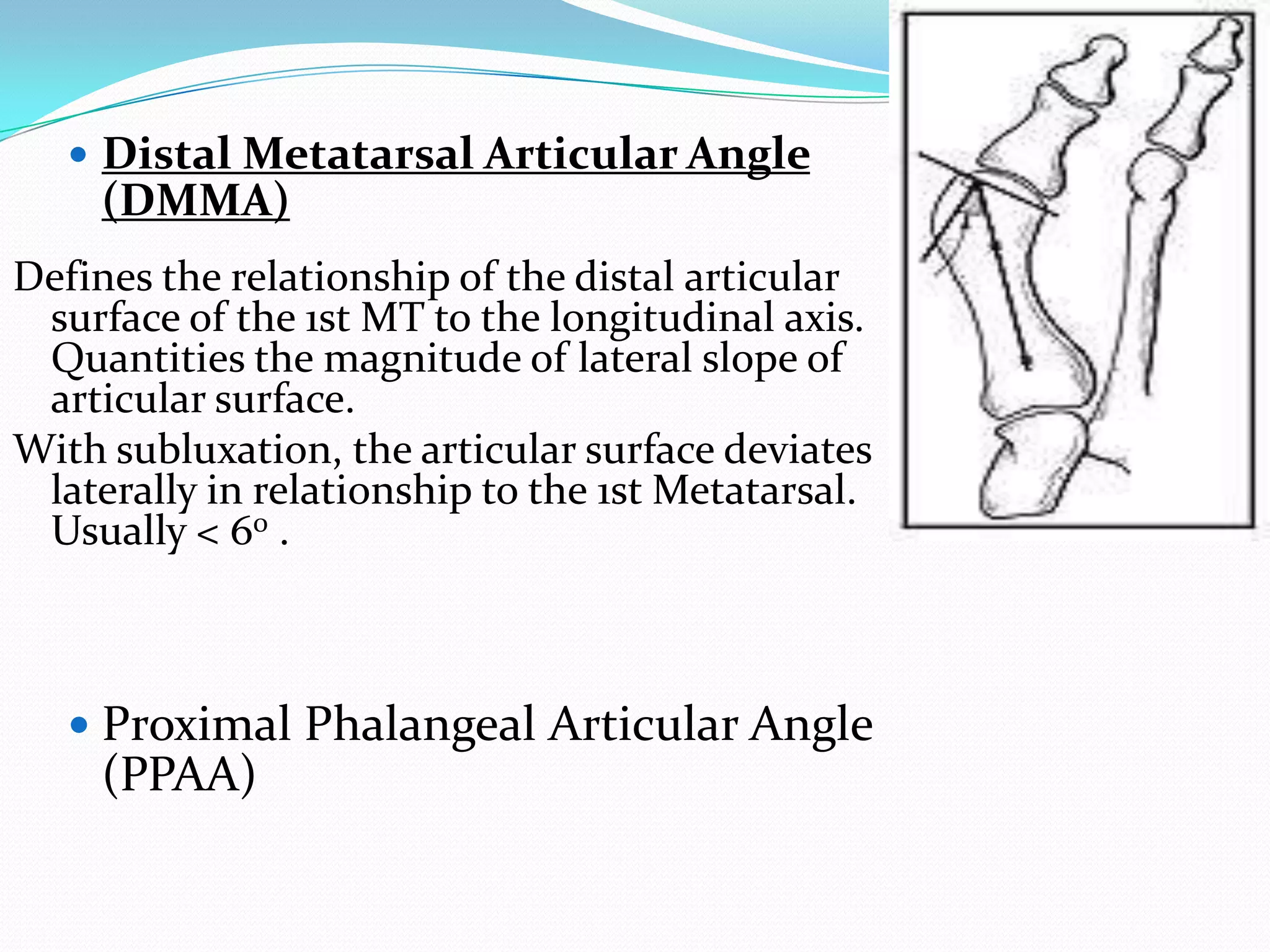
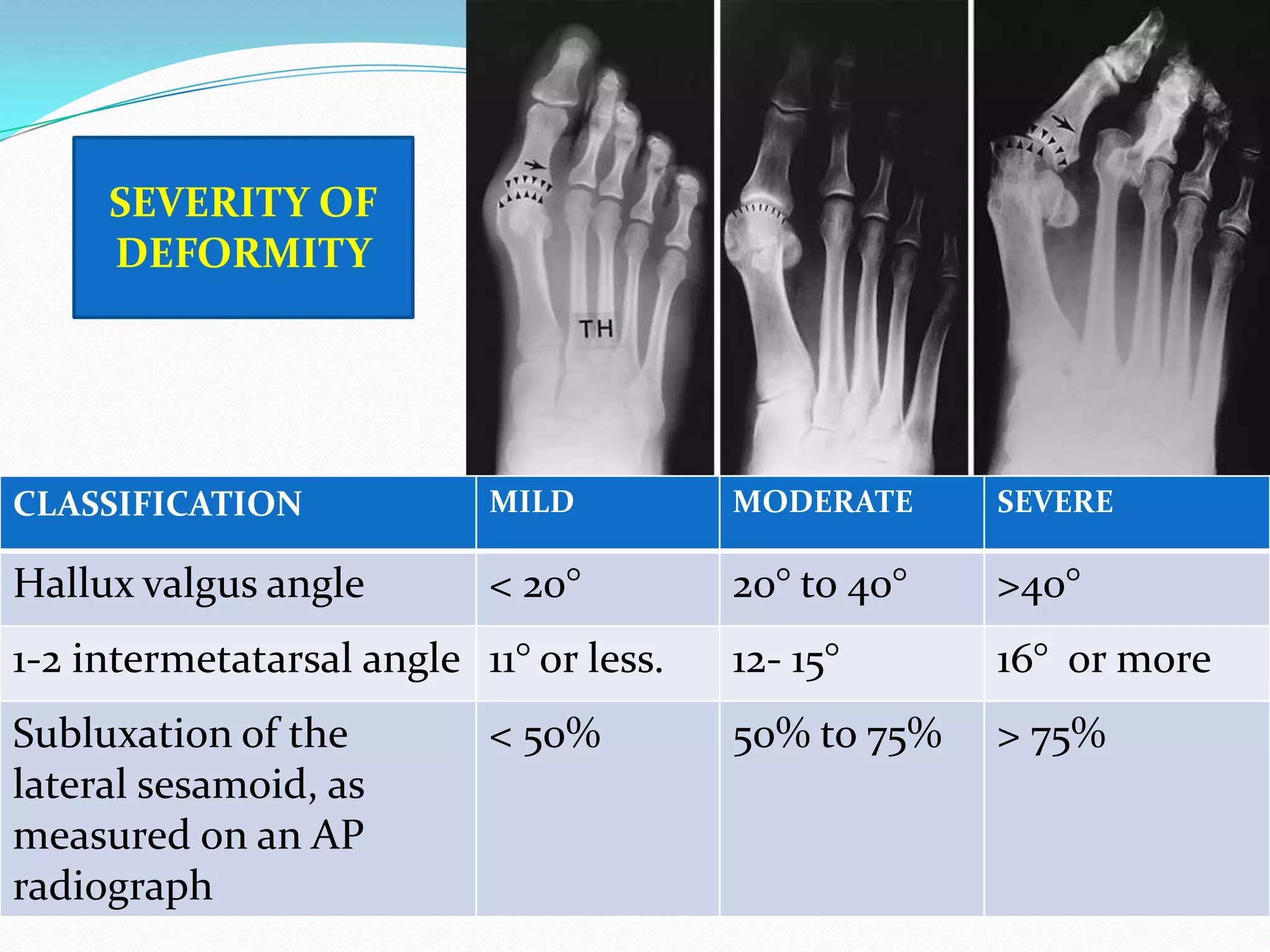
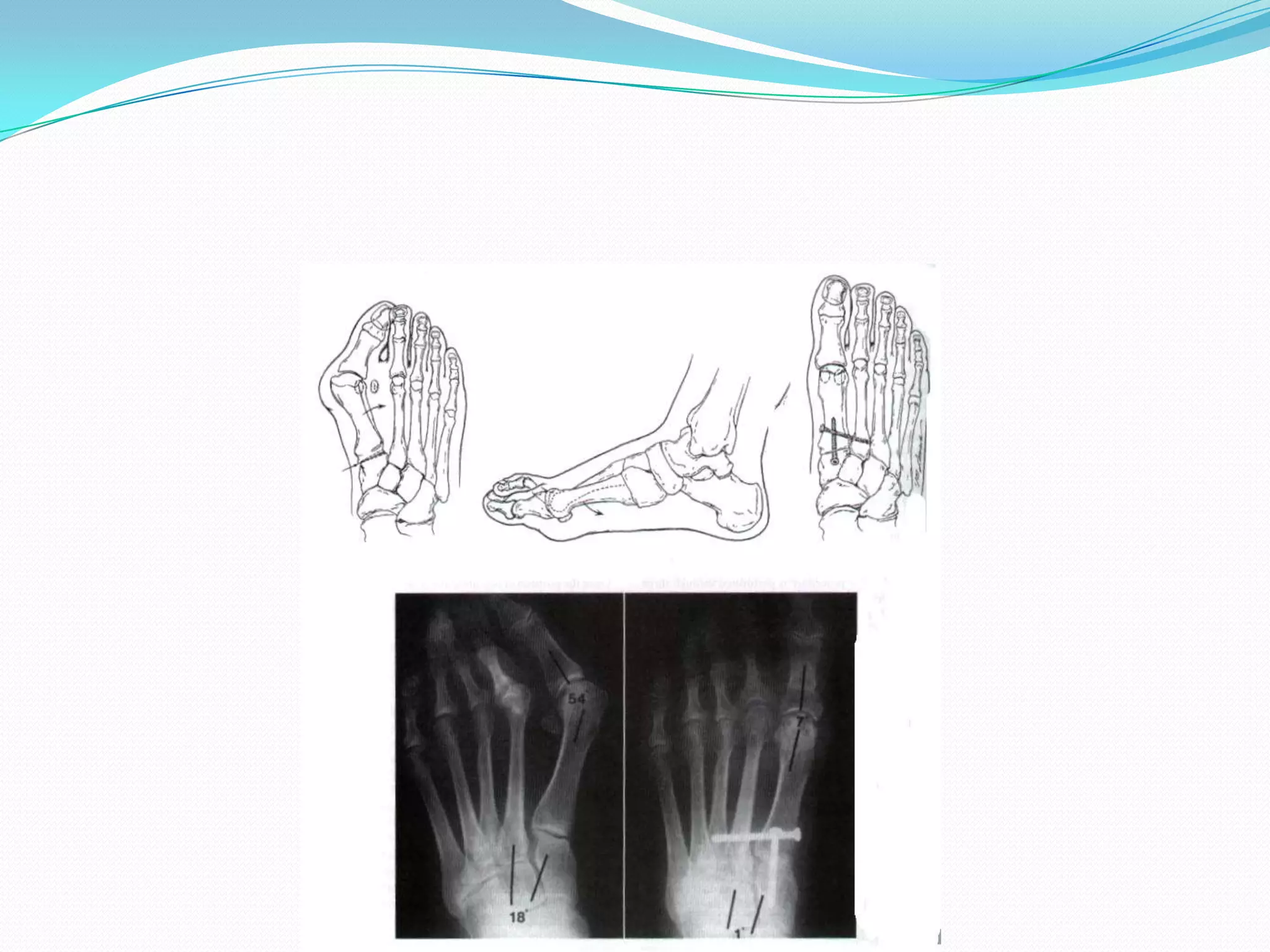
Measurement of hallux valgus angles; identifying severity via various angle metrics to assess metatarsal and phalangeal relationships.
Classification of hallux valgus severity based on angles, providing a systematic approach to assess the degree of deformity.
Treatment begins non-operatively; surgical options arise from persistent symptoms despite conservative measures.
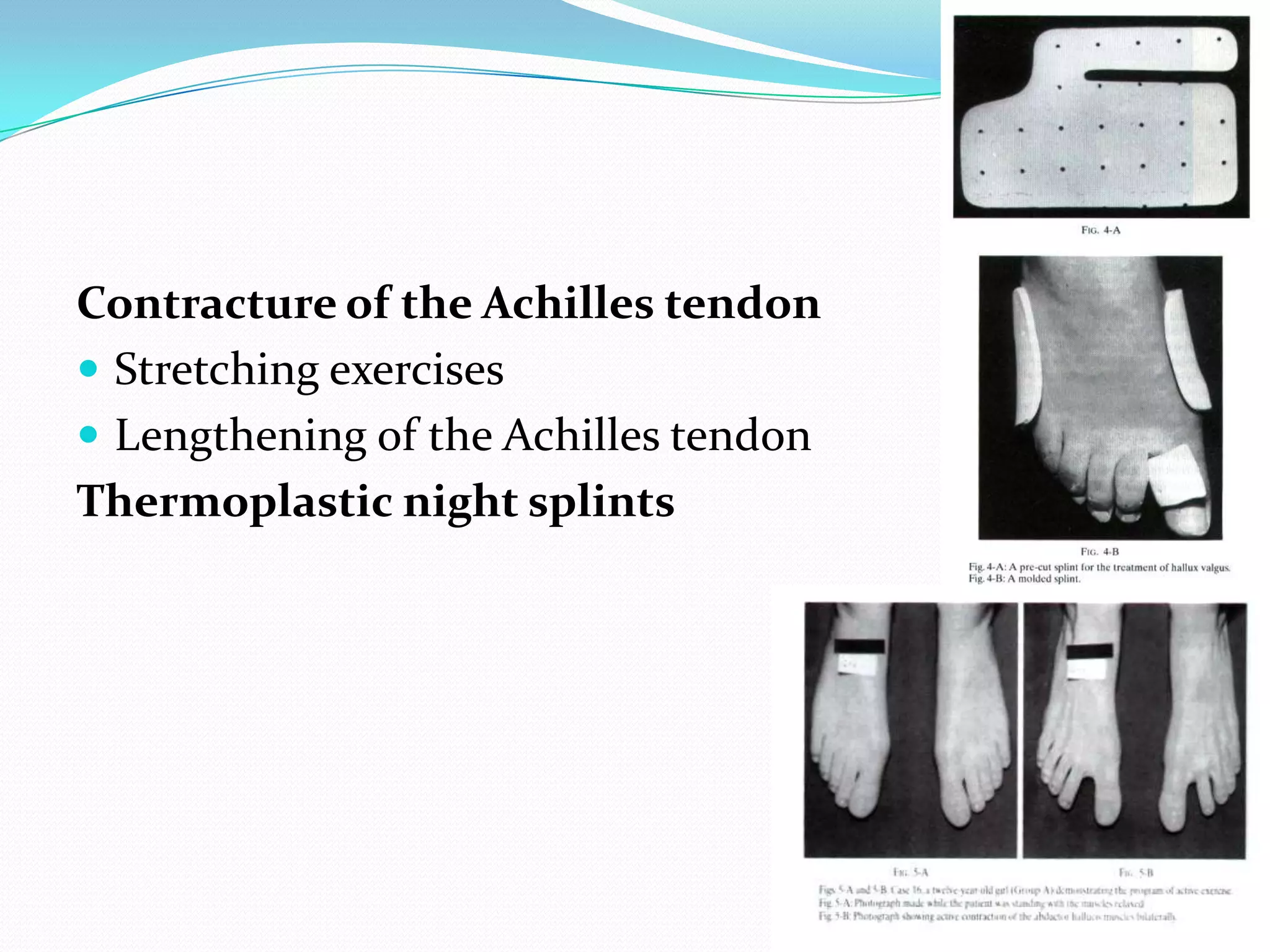
Non-surgical strategies include footwear modifications, stretching exercises, and use of thermoplastic splints for Achilles tendon issues.
Surgical treatment is indicated for persistent pain, deformation progression, and failure of non-surgical management.
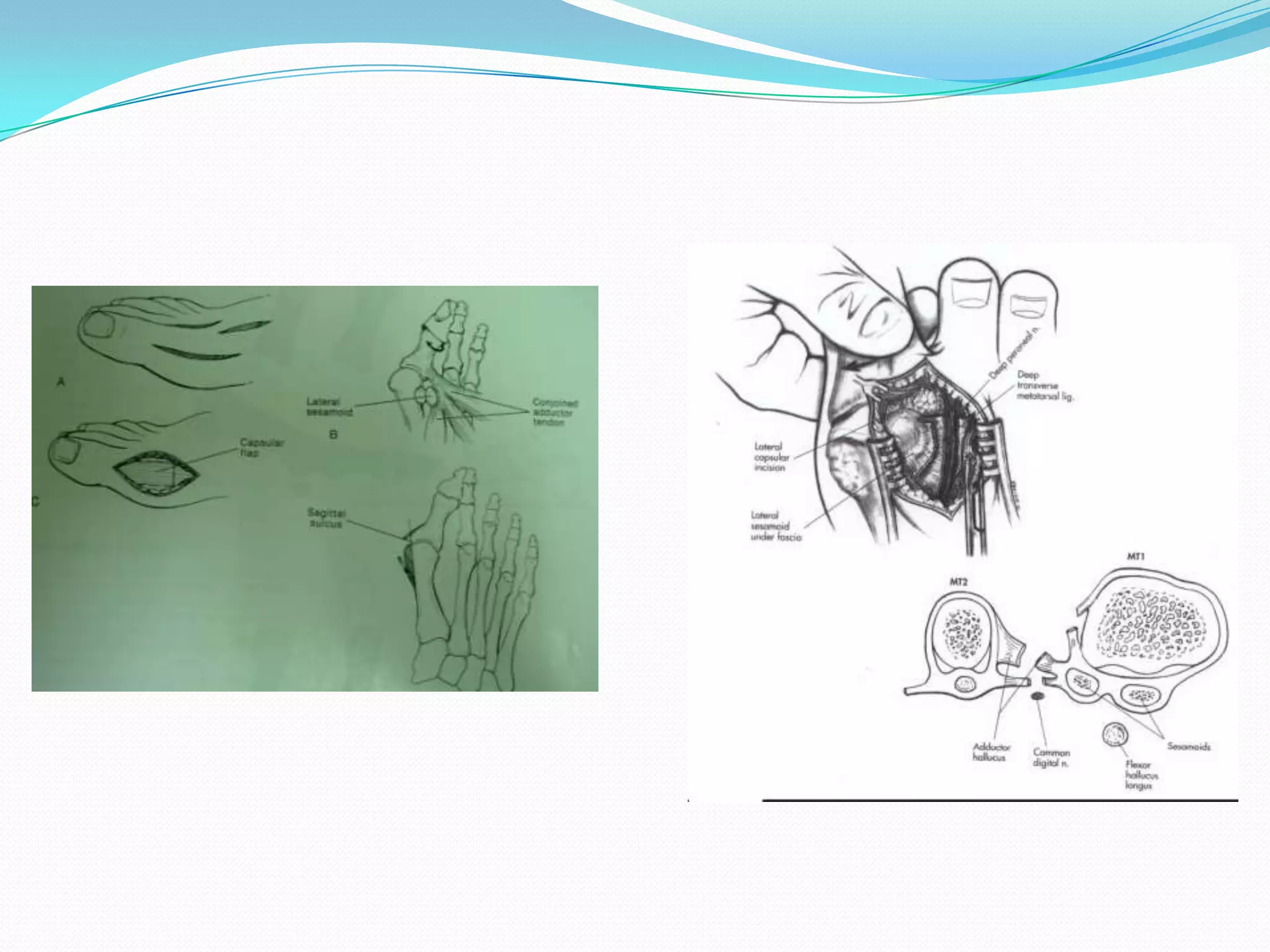
Soft tissue reconstructions with specific indications and constraints, emphasizing a combined approach to avoid recurrence.
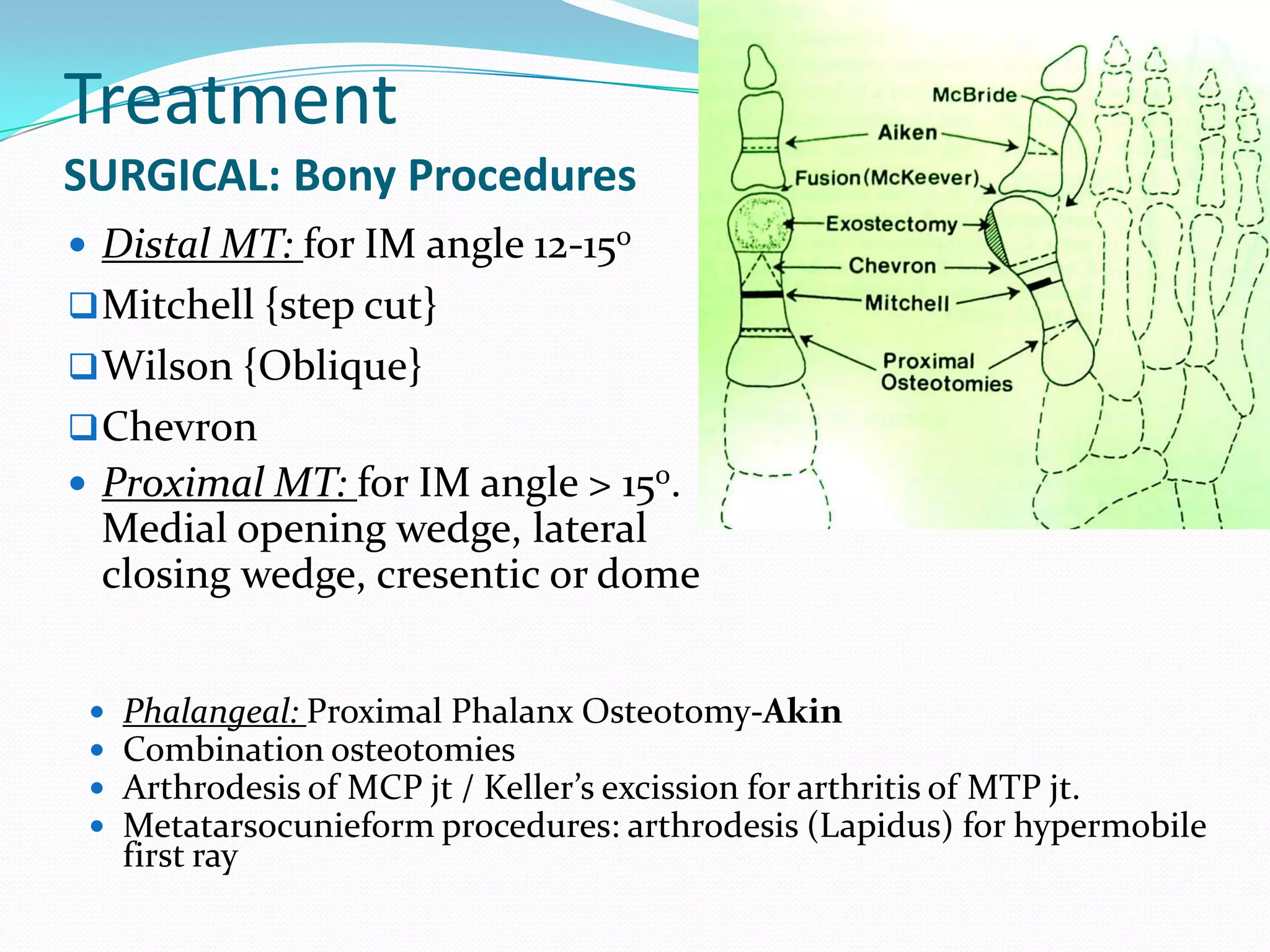
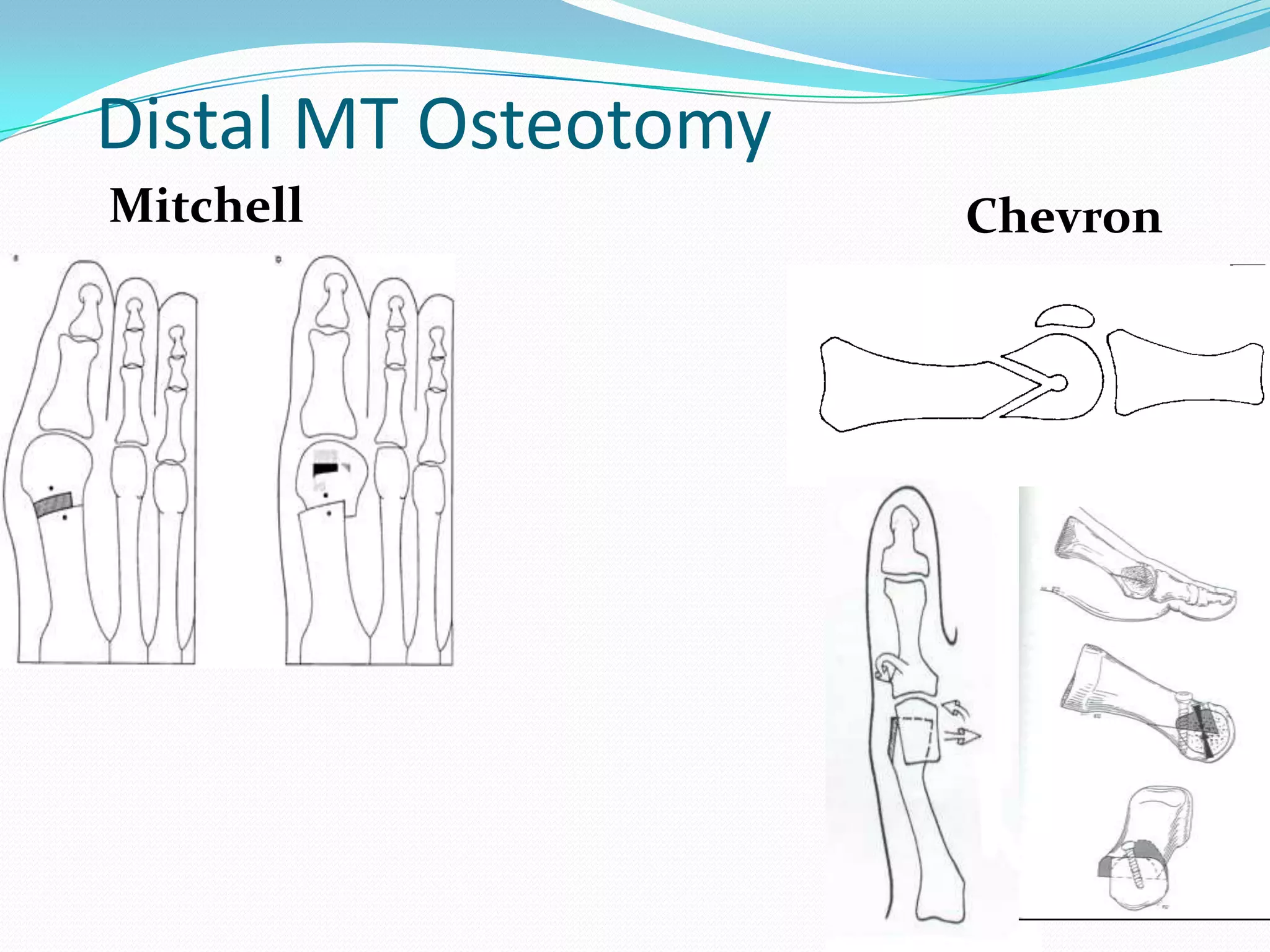
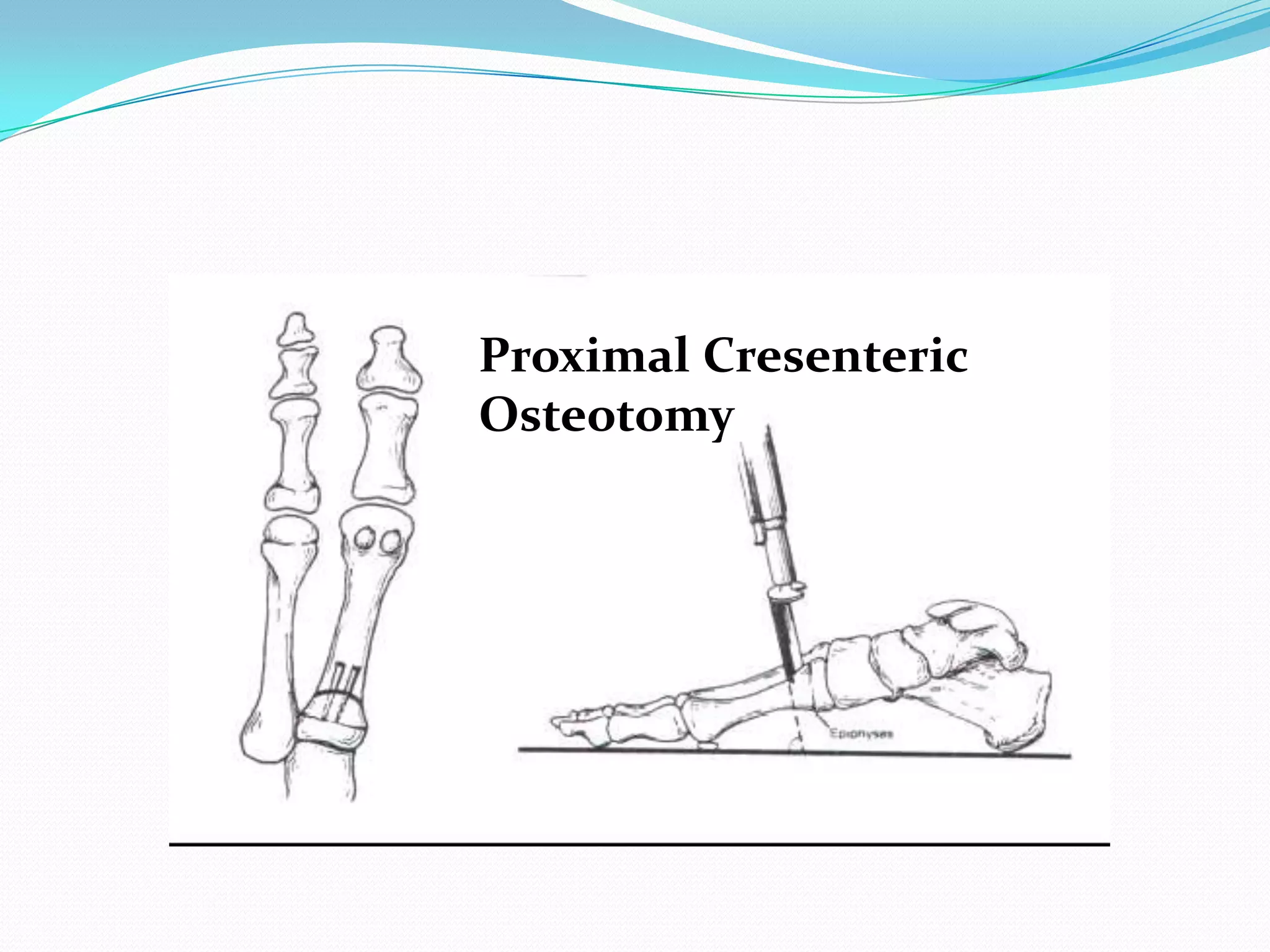
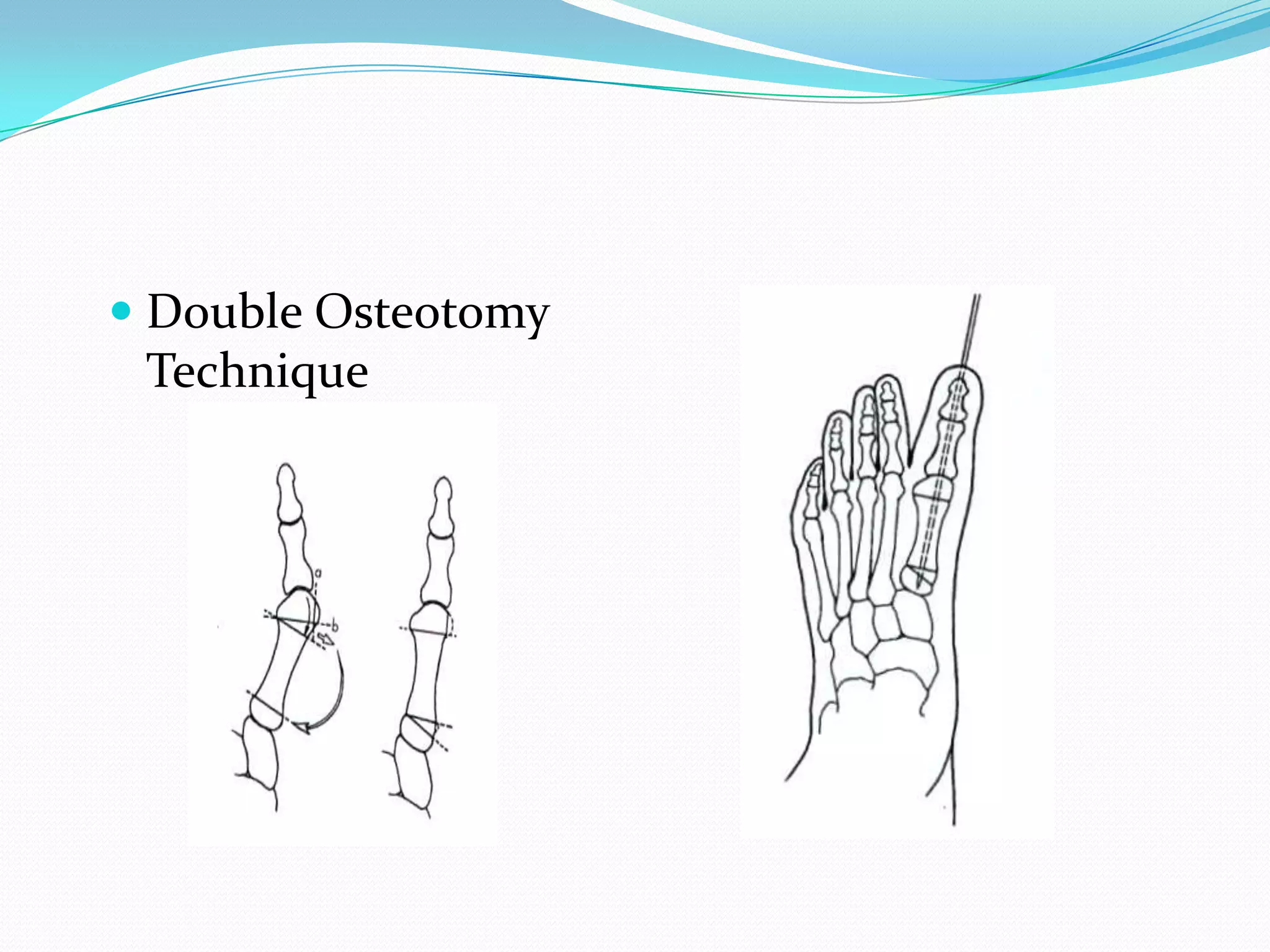
Discusses various osteotomy techniques to correct malalignment, detailing indications for both distal and proximal procedures.
Visuals of distinct osteotomy techniques such as Mitchell and Chevron to address angular deformities in hallux valgus.
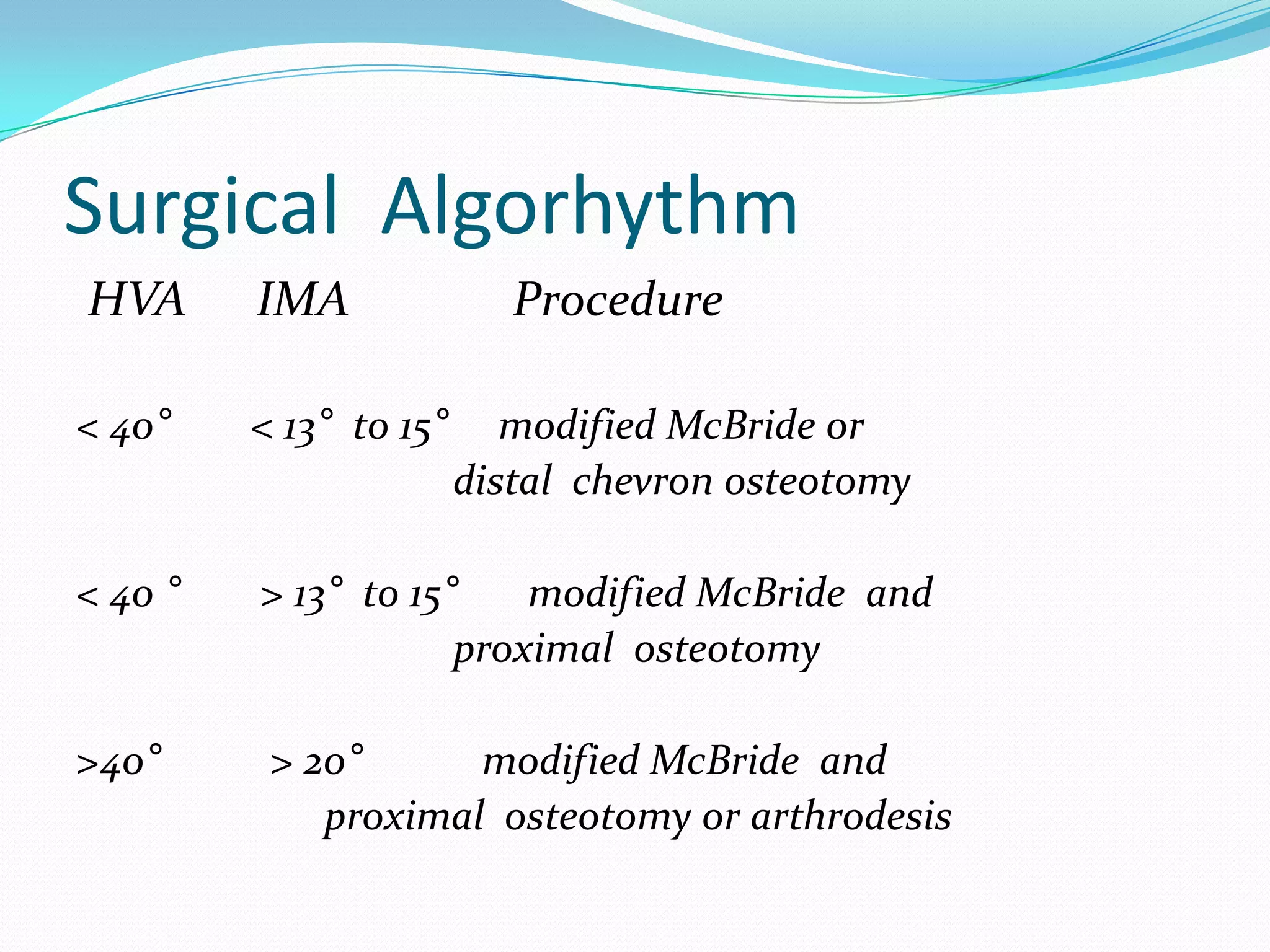
Algorithm detailing surgical procedures based on severity criteria including hallux valgus and intermetatarsal angles.
Potential complications following surgery, including recurrence, pain, neurologic injury, and nonunion/malunion risks.























































































