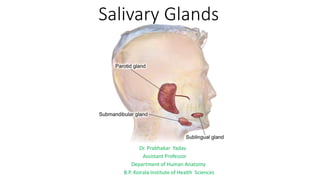
1. Salivary Glands
Dr. Prabhakar Yadav
Assistant Professor
Department of Human Anatomy
B.P. Koirala Institute of Health Sciences
2. Parotid Gland:
Largest salivary gland
Location: below external acoustic meatus,
between ramus of the mandible & sternocleidomastoid
Boundaries of the Parotid Bed (retromandibular fossa)
Anteriorly: Posterior border of ramus of mandible
Posteriorly: Mastoid process.
Superiorly: --External acoustic meatus &
--posterior part of temporomandibular joint.
Medially: Styloid process.
3. Muscles covering the Parotid bed :
Ramus of mandible : Masseter laterally & Medial pterygoid medially.
Mastoid process : Sternocleidomastoid laterally & Posterior belly of digastric muscle medially.
Styloid process : Styloglossus, Stylohyoid & Stylopharyngeus
Accessory parotid gland: Parotid extends over the masseter for a variable distance; often detached from the rest of
the gland.
• lies between the zygomatic arch & parotid duct. Several ducts from accessory gland open into the parotid duct.
4. Parotid Capsule:
True capsule: Condensation of fibrous stroma of the gland
False capsule: Investing layer of the deep cervical fascia forms a parotid capsule.
• Fascia splits between the angle of the mandible & mastoid process.
• Superficial lamina- thick & adherent to the gland; attached above to zygomatic arch.
• It blends with epimysium of masseter to form a parotidomasseteric fascia.
• Deep lamina is thin & is attached to tympanic plate and styloid process of temporal bone.
• portion of the deep lamina, extending between styloid process & mandible, is thickened- stylomandibular
ligament- separates parotid gland from submandibular gland.
5. Patey’s Faciovenous Plane:
Parotid gland is divided into large superficial & small deep lobes, connected by isthmus of the glandular tissue;
gland appears H-shaped in coronal section.
Plane between superficial & deep lobes - Patey faciovenous plane where lies the branches of facial nerves & veins
The plane is used by the surgeons to remove the parotid tumor.
6. External Features: 3 sided pyramid. Apex- directed downwards.
Four surfaces: (1) Superior (base of pyramid); (2) superficial; (3) anteromedial & (4) posteromedial.
Three borders: (1) Anterior (2) posterior & (3) medial
7. STRUCTURES PRESENT WITHIN THE PAROTID GLAND
From superficial to deep:
1. Facial nerve:
• Enters gland through upper part of its
posteromedial surface.
• Divides into its terminal branches within the gland.
• Branches leave the gland through its anteromedial
surface & appear on the surface at the anterior
border
2. Retromandibular vein:
• Formed within the gland by union of superficial
temporal and maxillary veins.
• In the lower part of the gland, the vein divides into
anterior & posterior divisions which emerge at
apex of the gland
8. External carotid artery:
• Enters gland through its posteromedial surface
• Maxillary artery leaves the gland through its anteromedial surface
• Superficial temporal vessels emerge at the anterior part of the
superior surface.
• Posterior auricular artery may arise within the gland.
Deep parotid lymph nodes & filaments of auriculotemporal
nerve are also located within the gland.
9. Parotid Duct (Stenson’s Duct): 5 cm long
• Emerges from the middle of the anterior border of the gland
• Runs forward over the masseter between upper & lower buccal branches of the facial nerve.
• At anterior border of masseter, turns inwards & pierces buccal pad of fat, buccopharyngeal fascia & buccinator
muscle
• Duct runs forwards (second bend) for about 1 cm between buccinator muscle & buccal mucosa.
• Finally, Duct turns medially (third bend) and opens into the vestibule of mouth opposite the crown of upper 2nd
molar teeth
10. VASCULAR SUPPLY
Arterial supply: External carotid & superficial temporal arteries.
Venous drainage: Retromandibular & External jugular veins.
LYMPHATIC DRAINAGE: superficial parotid lymph nodes (lie in the superficial fascia over the gland )&
Deep parotid lymph nodes ( lie deep to parotid capsule)
Finally drain into deep cervical lymph nodes.
11. Nerve Supply:
Parasympathetic nerves: are secretomotor fibre.
Reach the gland through auriculotemporal nerve.
Preganglionic fibres begin in inferior salivatory nucleus
pass through the glossopharyngeal nerve, its
tympanic branch (Jacobson’s nerve), tympanic plexus &
lesser petrosal nerve --- relay in otic ganglion.
Postganglionic fibres -- pass through auriculotemporal
nerve & reach the gland.
Sympathetic nerves: are vasomotor & are derived from the
plexus around the external carotid artery.
Sensory nerves:
to the gland - from auriculotemporal Nr.
parotid fascia- by sensory fibres of great auricular nerve
(C2).
Frey’s syndrome (auriculotemporal nerve syndrome):
12. Infection of the parotid gland by mumps virus causes
inflammationand swelling of the gland.
Parotid sialogram:
Parotid duct & its ramifications is demonstrated radiologically
by injecting radio-opaque dye through a fine needle into the
duct, in the vestibule of oral cavity
13. Sialolithiasis: Calculi (stones) may form in the parotid gland and parotid duct.
Calculi lodged in distal portion of the gland may be removed by splitting up the duct from its opening in the mouth
14. Mixed parotid tumour: is a slowly growing lobulated painless tumour without any involvement of the facial nerve.
Malignant change of such a tumour is indicated by pain, rapid growth, fixity with hardness, involvement of the
facial nerve & enlargement of cervical lymph Nodes
15.
16. Submandibular gland:
• Location: Anterior part of digastric triangle; J shaped
• Indented by posterior border of mylohyoid
• Larger superficial part superficial to the muscle & small deep part lying deep to muscle
17. Superficial Part
- is large & fills the anterior part of digastric triangle
- Extend upwards up to the mylohyoid line.
Three surfaces—Inferior, Lateral & Medial.
18. Gland is enclosed between two layers of investing layer of deep
cervical fascia.
At greater cornu of hyoid bone the investing layer of deep
cervical fascia splits into two laminae to enclose the superficial
part.
• Superficial layer covers the inferior surface of the gland & is
attached to the base of the mandible.
• Deep layer covers the medial surface of the gland and is
attached to the mylohyoid line of the mandible.
19. Relations
Inferior surface:
Skin.
Superficial fascia containing platysma & cervical branch of facial nerve.
Deep fascia.
Facial vein.
Submandibular lymph nodes.
20. Lateral surface is related to :
– Submandibular fossa of mandible.
– insertion of Medial pterygoid muscle
– Facial artery.
21. Medial surface :divided into three parts:
Anterior part is related to:
– Mylohyoid muscle.
– Mylohyoid nerve and vessels
– Submental branch of facial artery.
22. Medial surface :divided into three parts:
Middle (intermediate) part is related to:
– Hyoglossus muscle.
– Styloglossus muscle.
– Lingual and hypoglossal nerves.
– Submandibular ganglion.
23. Medial surface :divided into three parts:
Posterior part is related to:
-Styloglossus muscle.
-Stylohyoid ligament.
-Glossopharyngeal nerve.
-Wall of pharynx.
24. Deep Part
Lies deep to Mylohyoid & superficial to hyoglossus & styloglossus.
Posteriorly- is continuous with superficial part round the posterior border of the mylohyoid.
Anteriorly- extends up to posterior end of the sublingual gland
26. Submandibular duct (Wharton’s duct): 5 cm long
• Emerges at anterior end of the deep part
• Runs forwards on hyoglossus between lingual & hypoglossal Nr.
• Near anterior border ofhyoglossus, Duct is crossed by lingual Nr.
• Continues forward between sublingual gland & genioglossus.
• come lies just deep to the mucus membrane of the oral cavity.
• Opens in the oral cavity on the summit of a sublingual papilla at
the side of the frenulum of the tongue.
27. Calculi formation in submandibular gland and its duct
(Sialolithiasis) is more common than in the parotid duct
two reasons:
(a) Secretion is more viscid.
(b) Tortuous and upward course
Excision of the submandibular gland (for calculus or tumor):
Marginal mandibular branch of facial nerve passes one inch
posteroinferior to the angle of mandible before crossing its
lower border.
Incision should be given 4 cm below the angle to avoid injury
to this nerve.
28. Blood supply
Supplied by sublingual and submental arteries
Drained by common facial and lingual veins.
Lymphatic drainage
first drain into submandibular lymph nodes & subsequently into
jugulodigastric lymph nodes- (found in the proximity of where
posterior belly of digastric muscle crosses internal jugular vein.)
29. Nerve Supply:
1. Parasympathetic (secretomotor) supply:
• Preganglionic fibre arise from superior salivatory
nucleus in pons
• pass through facial, chorda tympani & lingual
nerves terminate in submandibular ganglion
• Postganglionic fibres from submandibular
ganglion supply submandibular gland.
2. Sympathetic (vasomotor) supply:
• Preganglionic fibres arise from T1 spinal segment
relay in superior cervical sympathetic ganglion
• Postganglionic fibres, form plexus around facial
artery, and reach gland through this artery.
3. Sensory supply: by lingual nerve.
30.
31. SUBLINGUAL GLAND
Lies in: sublingual fossa of the mandible; in the floor of the
mouth between mucus membrane & mylohyoid muscle.
Gland possesses about 20 ducts.
Most of these ducts (ducts of Rivinus) open separately on
the sublingual fold.
Ducts from anterior part of gland unite to form sublingual
duct (duct of Bartholin)- opens into submandibular duct.
32. Nerve supply:
Blood supply
sublingual & submental arteries.
Lymphatic drainage
drain into submental and submandibular lymph nodes.
Ranula: Mucus retention cyst in the floor of mouth
arising from sublingual salivary gland.
Swelling is soft, bluish in color & transilluminates