
Recommended
Recommended
More Related Content
Similar to Progress in Cardiovascular Nursing Winter 200818www.lejacq.docx
Similar to Progress in Cardiovascular Nursing Winter 200818www.lejacq.docx (20)
More from wkyra78
More from wkyra78 (20)
Recently uploaded
Recently uploaded (20)
Progress in Cardiovascular Nursing Winter 200818www.lejacq.docx
- 1. Progress in Cardiovascular Nursing Winter 200818 www.lejacq.com ID: 6611 Heart failure (HF) is the lead-ing cause of hospitalization for persons older than 65 years and often necessitates assistance from family caregivers.1,2 Approximately 40% of older adults are readmitted within 3 months postdischarge, resulting in significant health care costs.2,3 Indeed, more than one million hospitalizations attributed to HF cost the patient and United States health care system over $27 billion a year.1 Hospitalizations related to HF are complicated by the aging process, comorbidities, and psychosocial concerns that affect suc- cessful management.2 In a study of patient outcomes post– hospital discharge, Naylor and col- leagues4 demonstrated that the use of advanced practice nurses (APNs) was effective in improving outcomes for patients with HF. The feasibility of adapting this approach is limited, how- ever; costs for home visits by an APN are high, a shortage of APNs employed in home care exists, and funding for home care has decreased with the Medicare Prospective Payment System.5
- 2. An alternative strategy for promot- ing self-management of HF is the use of electronic home monitoring (EHM). EHM is a form of tele- medicine in which medical/nursing management interventions are pro- vided to individuals at a distance from the health care provider.6 The primary objective of this pilot study was to examine the effectiveness of postdischarge telemonitoring by an APN on reducing subsequent hospital readmissions, emergency department (ED) visits, and costs and increasing the time between discharge and read- mission among older adults with HF. Secondary objectives were to examine depressive symptomatology, quality of life, caregiver mastery, and social sup- port for patients with HF. BACKGROUND Older adults with HF face a high risk of early hospital readmission within 3 to 6 months of discharge.2,3 Upon hospital discharge, patients may encounter problems related to depressive symptoms, threatened quality of life, availability of informal and formal social support, and how they are monitored at home.2 Family caregiving is affected by how one copes with problems and resources available.
- 3. Researchers found that patients with cardiovascular disorders including HF have a high prevalence of depres- sive symptoms or feelings of hopeless- ness, with rates reported from 24% to >40%.7,8 Depressive symptoms were linked to increased hospital readmis- sions, number of comorbidities, impair- ment in activities of daily living, and the need for informal social support.7–9 HF has an enormous impact on the quality of life for patients because it is a chronic condition without a cure. According to the National Academy on an Aging Society,10 persons with heart disease are less satisfied with their lives than the general population. Heart failure (HF) is the leading cause of rehospitalization in older adults. The purpose of this pilot study was to examine whether telemonitoring by an advanced practice nurse reduced subsequent hospital readmissions, emergency department visits, costs, and risk of hospital readmission for patients with HF. One hundred two patient/caregiver dyads were randomized into 2 groups postdischarge; 84 dyads completed the study. Hospital readmissions, emergency department visits, costs, and days to readmission were abstracted from medical records. Participants were inter- viewed soon after discharge and 3 months later about effects of telemonitoring on depressive symptoms, quality of life, and caregiver mastery.
- 4. There were no signifi- cant differences due to telemonitoring for any outcomes. Caregiver mastery, infor- mal social support, and electronic home monitoring were not significant predictors for risk of hospital readmission. Further studies should address the interaction between the advanced practice nurse and follow-up intervention with telemonitor- ing of patients with HF to better target those who are most likely to benefit. Prog Cardiovasc Nurs. 2008;23:18–26. ©2008 Le Jacq From the College of Nursing, University of Akron, Akron, OH;1 the Department of Nursing, MetroHealth Medical Center, Cleveland, OH;2 and the Heart and Vascular Center, Akron General Medical Center, Akron, OH3 Address for correspondence: Karen A. Schwarz, PhD, RN, College of Nursing, University of Akron, Akron, OH 44325-3701 E-mail: [email protected] Manuscript received June 13, 2007; revised August 10, 2007; accepted August 16, 2007 P i l o t S t u d y Telemonitoring of Heart Failure Patients and Their Caregivers: A Pilot Randomized Controlled Trial Karen A. Schwarz, PhD, RN;1 Lorraine C. Mion, PhD, RN;2 Debra Hudock, MSN, RN;3 George Litman, MD3 Progress in Cardiovascular Nursing® (ISSN 0889-7204) is published Quarterly (March, June, Sept., Dec.) by Le Jacq, located at Three Enterprise Drive, Suite 401, Shelton, CT
- 5. 06484. Le Jacq is an imprint of Blackwell Publishing, which was acquired by John Wiley & Sons in February 2007. Blackwell’s programme has been merged with Wiley’s global Scientific, Technical, and Medical business to form Wiley-Blackwell. Copyright ©2008 by Le Jacq. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Ben Harkinson at [email protected] or 781-388-8511. ® Winter 2008 Progress in Cardiovascular Nursing 19 How patients adapt to a therapeutic regimen is strongly influenced by how they live within their disability.11 In one of the few published studies that has examined quality of life in patients with HF that received post–hospital discharge case management, Pugh and colleagues12 reported that quality of life scores were more favorable among those who received intensive postdis- charge collaboration with their provid- ers than those who received usual care. Furthermore, Goldberg and associ-
- 6. ates13 found that patients with HF who had access to in-home telemoni- toring had a slightly greater improve- ment in quality of life than those who received standard care. Caregiver mastery may be viewed as a personal resource that directly and indirectly affects the relationship between patient stressors and out- comes. Caregiving mastery includes the expectation that one is capable of coping with problems.14 In a rare study about caregiving skills, Scott15 related that caregivers of patients with HF described both positive and nega- tive components of receiving techno- logic care. While caregivers found sat- isfaction from caregiving, they feared the responsibilities of learning to use new technology. This learning may be associated with caregiver mastery. External resources in this study included informal social support pro- vided by family and friends and formal social support from home health care and EHM by an APN. Although fami- lies provide 80% to 90% of informal social support,16 there is a dearth of studies about the relationship of infor- mal social support and patient out- comes. Schwarz and Elman’s17 findings suggested that informal social support significantly reduced the risk of hos- pital readmission in patients with HF.
- 7. Formal social support such as home care is a vital resource for patients with HF because of the patient’s associ- ated functional decline and need for education. Stewart and colleagues18 reported that those patients receiving a structured home visit from a cardiac nurse 7 to 14 days after discharge had fewer unplanned hospital readmis- sions. Other researchers found that a comprehensive treatment program consisting of individualized home visits improved quality of life and decreased hospital readmissions and costs for patients with HF.19 An EHM system is typically moni- tored by an APN but does not replace direct home care visits. Rather, telem- onitoring provides more frequent (eg, daily) surveillance of important clini- cal parameters that allows for more rapid intervention, which theoretically in turn would delay or prevent ED visits and hospital admissions.20 Some researchers reported that the home telecare intervention had significantly reduced hospital readmissions, ED visits, and costs postdischarge.20–22 In addition, Roglieri and colleagues’23 findings indicated that a comprehen- sive program of patient education and telemonitoring by phone significantly reduced hospital admissions and read- missions. Using a daily EHM system,
- 8. Goldberg and coworkers13 found no significant differences in the overall time to death or first rehospitaliza- tion, however, and McManus24 found no significant differences in hospital readmissions that were attributed to telemonitoring. Although most of the previous studies were randomized con- trol trials,13,20,21,24 they differed on patient age, technology used to moni- tor patients, means of data collection, and analyses of data. Given the need to examine alterna- tive methods to survey and monitor patients with HF in the home in a time of limited health care person- nel, we examined the effectiveness of telemonitoring with an APN in a randomized clinical trial. The research hypotheses were as follows: - sions, ED visits, and costs of care will be significantly lower for HF patients with EHM as compared with usual care. symptoms will be lower, but days to readmission and measures of quality of life and caregiver mastery will be significantly higher in the EHM group compared with usual care. informal social support, and EHM
- 9. will significantly reduce the risk of hospital readmission for patients with HF. METHODS Setting and Sample This pilot study was conducted at a 537-bed tertiary teaching hospital in Northeastern Ohio. The study was reviewed and approved by the institutional review board at the participating hospital. Potential participants for the study included patient/caregiver dyads who met the following criteria and rou- tinely used the participating hospital. The patients, aged 65 years or older, had a diagnosis of New York Heart Association (NYHA) classification II, III, or IV HF25 and were functionally impaired in at least 1 activity of daily living (ADL) or one instrumental activity of daily living (IADL), neces- sitating assistance of a family caregiver. They received home care from the participating home care agency if it was ordered by their physician, had Medicare eligibility and an operat- ing telephone line, and were able to speak English. Classic symptoms of clinical HF are shortness of breath and fatigue, and abnormalities of systolic and diastolic dysfunction may coex- ist.25 The principal investigator (PI) validated the diagnosis of systolic and/
- 10. or diastolic HF with chart review of the cardiologist’s impressions related to signs and symptoms of HF, ejection fraction and/or the echocardiography report after gaining oral consent from the patient before hospital discharge. Exclusion criteria included planned discharge to a nursing home, inability to be interviewed because of physical illness, current use of a telemonitor- ing scale, inability to be contacted postdischarge, receiving regular infu- sions or dialysis, NYHA class I, inde- pendence in performing ADLs, no caregiver, use of hospice care, client of nonparticipating home health care Progress in Cardiovascular Nursing® (ISSN 0889-7204) is published Quarterly (March, June, Sept., Dec.) by Le Jacq, located at Three Enterprise Drive, Suite 401, Shelton, CT 06484. Le Jacq is an imprint of Blackwell Publishing, which was acquired by John Wiley & Sons in February 2007. Blackwell’s programme has been merged with Wiley’s global Scientific, Technical, and Medical business to form Wiley-Blackwell. Copyright ©2008 by Le Jacq. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Ben Harkinson at
- 11. [email protected] or 781-388-8511. ® Progress in Cardiovascular Nursing Winter 200820 agency, participation in another study, dementia, planned surgery, inability to speak English, planned hospitaliza- tion, and inability to stand on a scale. Inclusion criteria for caregivers includ- ed being cognitively intact, having a familial relationship to the patient, and providing assistance with at least 1 ADL or 1 IADL. Overall, 562 patients were screened for eligibility (Figure). Of these, 152 (27%) were eligible; 102 (67%) agreed to participate. Sample size determination was based on the reported difference (22%) in the proportion of patients readmitted in the control group vs the intervention group within 3 months of hospital discharge.19 The targeted enrollment was 84 patient/caregiver dyads using a power of 80% and a one-tailed test of significance with set at .05. Of the 102 dyads enrolled, 84 (82%) completed the study; 40 in the usual care group and 44 in the intervention group. Attrition was equivalent between groups.
- 12. Procedure Institutional review board approval was obtained, and cardiologists and internal medicine physicians gave written permission for their patients to be identified and enrolled. Potential participants were identified by the HF care manager with the assistance of care managers in 4 hospital units. While making daily rounds, the HF care manager informed potential participants about the study and gained oral permission for the PI to contact them before hospital discharge. Prior to discharge, the PI briefly explained the study to the patient and/or caregiver, provided a letter of explanation, and received oral consent for a chart review to verify whether they met study criteria. Patients provided their phone numbers for contact upon discharge. Participants were randomized to usual post–hospital discharge care or to usual care with a telemonitoring scale by drawing from a preprepared, sealed envelope. Participants were interviewed in their homes within 10 days of hospital discharge and 90 days later by trained registered nurses (RNs) who were not part of postdischarge care. To main- tain inter-rater reliability, checks were conducted periodically throughout the study and maintained at >90%
- 13. agreement. Written informed consent and Health Insurance Portability and Accountability Act (HIPAA) autho- rization were provided by patients and caregivers at the first interview. During data collection, patients received all standard treatments and services ordered by their primary phy- sicians/cardiologists. Participants randomized to the intervention group received the Cardiocom EHM system (Cardiocom, LLC, Chanhassen, MN) at the first interview, and the nurse removed the equipment 90 days later, at the sec- ond interview. The HF care manager trained the PI about use of the EHM system and ensured its availability. The RN data collector was further trained by the PI about the equipment and taught the patient/caregiver dyad how to use the EHM system. The PI met with the HF care manager weekly to discuss technical issues with the equipment. On occasion, the PI called patients soon after placement of the scales to inquire whether they had any difficulty understanding instructions for its use. EHM System The Cardiocom EHM system was leased to the research team during the study period, and patients were not responsible for charges. The RN data
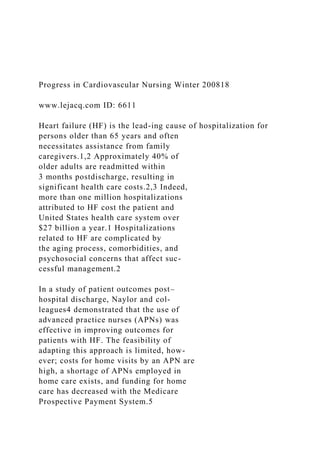
- 14. Hospitalized HF patients assessed for eligibility, N=562 Excluded, n=460 Refused, n=50 Ineligible, n=410 Nursing home, n=117 Too ill, n=97 Telemonitoring use, n=52 Inability to contact, n=40 Dialysis, infusions, n=28 Independent ADL, n=24 No caregiver, n=18 Hospice care, n=10 Non-agency client, n=8 In other study, n=6 Dementia, n=3 Need for surgery, n=2 Non–English speaking, n=2 Planned hospitalization, n=2 Unable to stand on scale, n=1 Randomized, n=102 Usual care, n=51 Usual care plus telemonitoring, n=51 Attrition Death, n=7
- 15. Nursing home, n=3 Withdrawal, n=1 Attrition Death, n=4 Nursing home, n=2 Withdrawal, n=1 Figure. Algorithm of study participants who were screened for eligibility. Progress in Cardiovascular Nursing® (ISSN 0889-7204) is published Quarterly (March, June, Sept., Dec.) by Le Jacq, located at Three Enterprise Drive, Suite 401, Shelton, CT 06484. Le Jacq is an imprint of Blackwell Publishing, which was acquired by John Wiley & Sons in February 2007. Blackwell’s programme has been merged with Wiley’s global Scientific, Technical, and Medical business to form Wiley-Blackwell. Copyright ©2008 by Le Jacq. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Ben Harkinson at [email protected] or 781-388-8511. ® Winter 2008 Progress in Cardiovascular Nursing 21
- 16. collector placed a weight scale in the participants’ homes and connected via the telephone line to a computer system in the collaborating hospital. The data-receiving computer was positioned in an office on the telemetry unit of the study hospital. The EHM system was programmed to measure weight on a daily basis. The display on the device asked the participants to answer “yes” or “no” to questions about shortness of breath, cough, fatigue, swelling, chest discomfort, urination, exercise, dizziness, medication use, and sodium intake. The computer stored each patient’s electronic health file and automatically displayed clinical variances when prescribed parameters exceeded predetermined ranges. Variances included failure to call daily, changes in symptoms, and weight outside prescribed parameters. The Cardiocom Telescale (Cardiocom, LLC, Chanhassen, MN) is accurate to ±0.1 lb and detects as little as 45 mL of fluid gain (D. Consentino, oral communication, February 8, 2002). The HF care manager, an APN, was responsible for daily monitoring of parameters received electronically. When participants had measurements outside of prescribed parameters, the monitoring nurse called the caregiver in the dyad to further assess the situation, provide education, and update the
- 17. medication regimen. In addition, the APN notified the primary physician or cardiologist about the patient’s status as needed. Variables and Measures Demographics such as age, sex, education, race, socioeconomic status, and perceived health of the patient and caregiver were measured by self-report at baseline. Hospital readmissions, defined as unplanned hospital readmissions for HF symptoms within 3 months post–hospital discharge, were collected by medical record review after 90 days postdischarge. Emergency department visits for HF were ascertained through medical record review after 90 days’ postdischarge. Days to readmission were used as a measure of risk for hospital readmission. Days to readmission, defined as the number of days between the date of initial hospital discharge and the first readmission to the hospital, was assessed through medical record review after 90 days’ postdischarge. Physiologic health indicators, blood pressure, apical pulse, weight, and oxy- gen saturation were assessed by the PI or research RN at baseline and 3 months later. Comorbidities and pre- scribed medications were abstracted from the medical record before hos- pital discharge and were confirmed at
- 18. baseline. Use of home health care was documented with a computerized chart review after 90 days’ postdischarge. Severity of HF was assessed subjectively by the PI or research RN using the NYHA functional class25,26 at baseline and at 90 days’ postdischarge. Functional status was measured as the ability to perform ADLs and IADLs at baseline and 90 days’ post- discharge. The ADL tool27 consists of 6 items (eating, dressing, bathing, transfers, incontinence, and toileting) and is scored from 0 (totally indepen- dent) to 2 (totally dependent). The ADL Index has a Cronbach’s of 0.82 for hospitalized older adults.28 Seven items from the IADL scale29 (eg, cooking, housekeeping) were scored similarly. The IADL scale has a high reproducibility coefficient of 0.96 and inter-rater reliability of 0.87.29 The ADL and IADL sum score range is 0 to 26. Spector and Fleishman30 demonstrated the feasibility and valid- ity of combining the 2 scales with a sample of functionally disabled older adults and reported that the correla- tion between the IADL scores and ADL scores was 0.70. For this sample, Cronbach’s was 0.85 for the com- bined scale. Depressive symptomatology was measured using the Center for
- 19. Epidemiological Studies Depression Scale (CES-D)31 at baseline and 90 days’ postdischarge. Participants rated 20 items on a 4-point Likert scale from 0 (“rarely”) to 3 (“most or all of the time”) with a possible range of 0 to 60. Higher scores indicate more depressive symptoms. The CES-D demonstrated excellent psychometric properties in community samples.31,32 In this sample, Cronbach’s at time 1 and time 2 were 0.89. Quality of life, defined as patient’s perceptions of the effects of HF on one’s life, was measured with 18 items from the Minnesota Living with HF questionnaire (MLWHF)11,33 at base- line and 90 days’ postdischarge. The MLWHF measures individuals’ percep- tions of the ways in which symptoms of HF have impacted their lives in the past month. Since the majority of patients were older and not employed and depression was assessed with the CES-D, questions about working, sexual activities, and depression were eliminated from the original scale. Eighteen items were rated on a 6-point Likert scale from 0 (“no”) to 5 (“very much”), with a possible range of 0 to 90. A higher score indicated more symptomatic impact on one’s life. For this sample, Cronbach’s coefficients at time 1 and time 2 were 0.91. Rector
- 20. and Cohn33 reported that the MLWHF was a valid patient self-assessment of the therapeutic benefit of medical therapy. Caregiver mastery, defined as a positive view of one’s ability to provide care, was measured with the mas- tery subscale from the Philadelphia Geriatric Center Caregiving Appraisal Scale (PGCCAS)34 at baseline and 90 days’ postdischarge. Six items assess the likelihood of caregiver uncertainty about how to provide care, reassurance that the patient is receiving proper care, feeling on whether they should be doing more for the patient, feel- ing that they are doing a good job of providing care, perceptions about capability of dealing with problems as they arise, and identifying the patient’s needs. Caregivers rated 6 items on a 5-point Likert scale from 1 (“never”) to 5 (“nearly always”), with a possible range of 6 to 30. Higher scores indi- cated greater mastery. Studies demon- strated moderate Cronbach’s coeffi- cients ranging from 0.61 to 0.73.34,35 For this sample, Cronbach’s was 0.65 at time 1 and 0.70 at time 2. Progress in Cardiovascular Nursing® (ISSN 0889-7204) is published Quarterly (March, June, Sept., Dec.) by Le Jacq, located at Three Enterprise Drive, Suite 401, Shelton, CT 06484. Le Jacq is an imprint of Blackwell Publishing, which was acquired by John Wiley & Sons in February 2007. Blackwell’s programme
- 21. has been merged with Wiley’s global Scientific, Technical, and Medical business to form Wiley-Blackwell. Copyright ©2008 by Le Jacq. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Ben Harkinson at [email protected] or 781-388-8511. ® Progress in Cardiovascular Nursing Winter 200822 Informal social support, described as instrumental activities performed by families and friends, was mea- sured with the tangible subscale from the Modified Inventory of Socially Supportive Behaviors Scale (MISSB)36 at baseline. The tangible subscale reflects activities such as receiving a monetary loan. Caregivers rated 9 items on a 4-point Likert scale from 1 (“never”) to 4 (“very often”), with a possible sum score of 9 to 36. Higher scores indicated more informal social support. Cronbach’s coef- ficients ranged from 0.71 to 0.92 in studies of caregivers of patients who
- 22. were recently hospitalized.17,32 For this sample, the Cronbach’s coefficient was 0.90. Cost of care was calculated for the 90-day period post–initial hospital- ization. Charges posthospitalization were calculated by tracking billing charges for rehospitalization, emer- gency department visits, and charges for usual home care from the provider of home health care. Costs of care for the EHM group included the former charges plus the additional monthly charge of renting the monitoring sys- tem. Charges for usual home care were calculated by multiplying the stan- dard charge data times the number of visits by the RN (at $155 per visit), home health aide (at $85 per visit), social worker (at $165 per visit), and physical therapist, occupational thera- pist, dietitian, or speech therapist (at $140 per visit). Supply costs averaged $38.50 per episode of care. Charges for EHM were calculated for direct costs of placement of the Cardiocom unit ($165). Data for reimbursement for the telemonitoring specialist were not available and, therefore, not included. In addition, out-of-pocket expenses for services posthospitalization were determined by calculating the number of physician office visits and instances of laboratory work and assigning a co-
- 23. pay of $12. Data Analyses Descriptive and comparative analyses were performed using SPSS for windows, version 13 (SPSS, Inc, Chicago, IL). Descriptive statistics, frequencies, and measures of central tendency and dispersion were used to describe the sample. Associations between variables were analyzed with Pearson correlation coefficients for interval variables and the Spearman correlation coefficient for ordinal variables. Means were substituted for the relatively few areas of missing data. The effectiveness of the intervention was examined by using an intention- to-treat analysis; was set at ≥.05. Outcomes were examined between the 2 groups using chi-squared likelihood ratio tests for categorical variables, t tests for approximately normally distributed variables, and Wilcoxon rank sum tests for skewed variables. Subgroup analyses were conducted, comparing the intervention and usual care groups by risk status. Survival analysis with Cox propor- tional hazard modeling37 was used to assess risk for hospital readmission by the number of days between discharge and first readmission. Cox proportional hazard modeling accommodates for the
- 24. Table I. Participant and Caregiver Characteristics at the Index Hospital Visit by Study Group (N=102) PATIENT INTERVENTION GROUP (N=51) USUAL CARE GROUP (N=51) P VALUE Age, y 77.1±7.3 79.1±6.9 .17 Femalea 22 (43) 31 (61) .07 Whitea 41 (80) 42 (82) .56 Marrieda 36 (71) 28 (55) .25 High school graduate or highera 42 (82) 25 (49) .01 ADLb/IADLc 6.5±4.9 8.1±4.1 .08 NYHA class IIa 12 (24) 9 (18) .74 NYHA class IIIa 23 (45) 26 (51) NYHA class IVa 16 (31) 16 (31) Comorbidities 4.2±2.4 4.9±2.1 .14 Current medications 10.2±4.5 9.9±3.7 .79 Heart medications 5.6±1.9 5.4±2.0 .51 Cardiologista 46 (90) 41 (80) .16 CAREGIVER Age, y 63.9±15.4 63.0±16.7 .76 Relationship .12 Spousea 32 (64) 22 (43) Childa 13 (26) 16 (31) Othera 5 (10) 13 (26) Values are expressed as mean ± SD unless otherwise indicated. aValue is No. (%). bFunctionally impaired in >1 activity. cFunctionally impaired in 1 activity. Abbreviations: ADL, activities of daily living; IADL, instrumental activities of daily living; NYHA, New York Heart Association. Progress in Cardiovascular Nursing® (ISSN 0889-7204) is published Quarterly (March, June, Sept., Dec.) by Le Jacq, located at Three Enterprise Drive, Suite 401, Shelton, CT 06484. Le Jacq is an imprint of Blackwell Publishing, which
- 25. was acquired by John Wiley & Sons in February 2007. Blackwell’s programme has been merged with Wiley’s global Scientific, Technical, and Medical business to form Wiley-Blackwell. Copyright ©2008 by Le Jacq. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Ben Harkinson at [email protected] or 781-388-8511. ® Winter 2008 Progress in Cardiovascular Nursing 23 censoring of information and accounts for the competing risk.17,37 The pool of potential predictors of risk for hospital readmission specific to the dyad includ- ed caregiver mastery, informal social support, and EHM. The multivari- able model was derived using multiple model building techniques: backward elimination with =.05 stay criteria, stepwise with =.25 enter criteria, and =.05 stay criteria to identify indepen- dent predictors of days to readmission.
- 26. RESULTS Participant Profile One hundred two patients were originally enrolled in the study; 51 in the EHM group and 51 in the usual care group. The mean age of the entire sample was 78.1 years with a range of 65 to 94 years. Fifty-two percent (n=53) were women. Participant characteristics at the time of the baseline visit in the hospital are shown in Table I. Education level was significantly higher for patients in the intervention group ( 2=18.5; P=.01). At baseline and 3 months later, there were no significant differences between groups for prescribed use of angiotensin-converting enzyme inhibitors, -blockers, digoxin, or diuretics. Twenty percent of the participants (n=20) had implanted defibrillators. Significant differences existed for use of defibrillators between the inter- vention (n=14) and usual care (n=6) groups at baseline ( 2=3.98; P=.05). At 90 days’ postdischarge, differences for defibrillators were similar between the intervention (n=13) and usual care (n=6) groups ( 2=2.53; P=.11). Twenty percent of patients without defibrillators did not finish the study. The number of hospital readmissions was similar between those with and without defibrillators (t=–1.3; P=.19).
- 27. Use of home care, total number of home care services, and informal social support were similar between inter- vention and usual care groups (P=.32, .66, and .74, respectively). The total sample reported having multiple comorbidities: hypertension (51%), diabetes (50%), atrial fibril- lation (30%), myocardial infarction (29%), stroke (13%), bypass surgery (28%), chronic obstructive pulmo- nary disease (29%), and cancer (6%), and groups had similar comorbidi- ties ( 2=12.13; P=.28). Systolic blood pressure at baseline ranged from 84 to 180 mm Hg with a mean of 127.56±19.21 mm Hg, and diastolic blood pressure ranged from 50 to 100 mm Hg with a mean of 69.3±9.74 mm Hg. Heart rate ranged from 40 to 110 beats per minute (bpm) with a mean of 71.39±11.4 bpm. Oxygen saturation ranged from 86% to 98% with a mean of 94.9±2.36%. Weight ranged from 85.6 to 372.5 lb with a mean of 179.14±49.53 lb. Caregivers reported providing assistance from 1 month to 27 years with a mean of 4.5±5.5 years. Patient/caregiver dyads that com- pleted the study (n=84) did not differ from those who did not (n=18) on demographic characteristics, physi- ologic health indicators, severity of
- 28. illness, depressive symptomatology, quality of life, informal social sup- port, caregiver mastery, or cognition. Patients not completing the study were more dependent in ADLs and IADLs than those who completed it (10.8±4.1 vs 6.6±4.3; t=–3.67; P<.001). Electronic Home Monitoring The majority of participants in the intervention group (91%) reported using the EHM system on a daily basis during the 90-day post–hospital discharge monitoring period. According to the APN’s report, however, the majority of patients (93%) did not use the EHM system on at least 1 day. The mean number of days that EHM system was not used was 16.1±17.9 days for the investigation group with a range of 0 to 66 days. The APN called the majority of patients (95%) about symptoms that exceeded the parameters on at least 1 day during the 90-day monitoring period. The average number of days that the APN called patients in the intervention group who reported symptoms that exceeded the prescribed parameters was 26.7±21.14 with a range of 0 to 77 days. Hospital Readmissions, Emergency Department Visits, and Costs of Care Between Groups
- 29. Table II displays subsequent hospital readmissions, emergency department visits, and costs 90 days’ postdischarge. There was no difference in hospital readmission between the intervention (n=12) and usual care (n=13) groups ( 2=0.27; P=.60). Hospital charges alone did not differ significantly between intervention and usual care groups ($10,996.86±$29,230.05; $5,462.58±$9,825.00, respectively; P=.26). In addition, out-of-pocket costs for medications, physician office visits, and laboratory testing were similar between groups. Depressive Symptoms, Days to Readmission, Quality of Life, and Caregiver Mastery Between Groups Table III displays depressive symptoms, days to readmission, quality of life, and caregiver mastery among the intervention and usual care groups at 90 days’ postdischarge. While differences existed between groups Table II. Subsequent Hospital Readmission, ED Visits, and Cost of Care by Group (N=84) VARIABLE INTERVENTION GROUP (N=44) USUAL CARE GROUP (N=40) P VALUE Hospital readmission 0.32±0.6 0.33±0.6 .90 ED visits 0.34±0.6 0.38±0.5 .73 Costs of care, US $ 12,017.99±29,405.65 6,673.29±10,258.28 .28 Values are expressed as mean ± SD. Abbreviation: ED, emergency department.
- 30. Progress in Cardiovascular Nursing® (ISSN 0889-7204) is published Quarterly (March, June, Sept., Dec.) by Le Jacq, located at Three Enterprise Drive, Suite 401, Shelton, CT 06484. Le Jacq is an imprint of Blackwell Publishing, which was acquired by John Wiley & Sons in February 2007. Blackwell’s programme has been merged with Wiley’s global Scientific, Technical, and Medical business to form Wiley-Blackwell. Copyright ©2008 by Le Jacq. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Ben Harkinson at [email protected] or 781-388-8511. ® Progress in Cardiovascular Nursing Winter 200824 at baseline with regard to caregiver mastery, there were no differences between groups for any outcome at the 90-day follow-up visit. For those readmitted to the hospital, days to readmission were similar between the intervention and usual care group (40.6±31.3; 41.2±24.0, respectively; P=.96). For the entire sample, quality
- 31. of life improved significantly from baseline to the 90-day follow-up visit (t=3.9; P<.0001). Caregiver Mastery, Informal Social Support, and Telemonitoring as Predictors of Reduced Hospital Readmission Cox proportional hazards regression modeling was used to identify independent predictors of risk for hospital readmission in days. Independent variables included caregiver mastery, informal social support, and telemonitoring (yes/ no). None of these predicted risk of hospital readmission. DISCUSSION Aging of the US population and concomitant increase in the prevalence of HF dictate the need for strategies to improve self-care management and minimize costly health service utilization. This pilot study examined whether the addition of an EHM system and APN responder to usual postdischarge home care would reduce number of hospital readmissions, emergency department visits, health service charges, and risk of readmission among older patients with HF. In addition, we examined whether more frequent surveillance and contact with patients and their caregivers would
- 32. decrease depressive symptoms, increase days to readmission, improve quality of life, and increase caregivers’ sense of mastery in the management of HF. We found no significant health care consumption or psychological benefit to patients by adding telemonitoring in the health service. The overall lack of effect of our intervention might be related to several issues, including the experience of the current cohort of older adults and the nature of their illness. Baby boomers are more experienced with technology and they may desire more sophisticat- ed means of monitoring their health as they age. A higher proportion of our patients (79%) were classified as NYHA class III or IV as compared with an earlier study by Schwarz and Elman.17 Newer therapies added to traditional medical therapy have led to improvements in function, exercise capacity, and quality of life in many studies of patients with mild to mod- erate HF.25 In this study, equivalency in hospital readmission and emer- gency department visits among groups may reflect the natural history of HF for patients with a clinically advanced state.13 Management of HF is further compounded by many psychosocial and economic factors that cannot always be measured.2 Furthermore,
- 33. since the APN was not always avail- able on weekends, monitoring by phone may have varied within the intervention group. Although Jerant and associates20 and Benatar and colleagues21 found that telemonitoring reduced hospital readmissions and emergency depart- ment visits, our findings are consistent with the lack of effect of telemoni- toring found by Goldberg and col- leagues13 and McManus.24 Compared with the reports of Jerant and cowork- ers20 and Bentar and colleagues,21 our patients were older and may have had less chance to respond optimally in the short follow-up time. Jerant and asso- ciates20 followed patients for 180 days; thus, a 90-day follow-up may not have been adequate to educate patients and their caregivers about self-care and adherence to the plan of care. Similar to Pugh and colleagues’12 findings but contrary to others,20–22 costs post–hospital discharge did not differ significantly between groups. For the present study, a member of the research team was able to access hospitalization costs for readmissions. Costs were not categorized by physi- cian visits, supplies, tests, etc. Although telemonitoring did not save on costs for health services, costs related to saving
- 34. Table III. Depressive Symptoms, Days to Readmission, Quality of Life, and Caregiver Mastery at 90 Days by Study Group VARIABLE INTERVENTION GROUP (N=44) USUAL CARE GROUP (N=40) P VALUE Depressive symptoms At baseline 8.7±8.9 6.8±8.9 .32 At 90 days 8.2±11.2 6.6±6.7 .44 Days to readmission At baseline At 90 days 40.6±31.3 41.2±24.0 .96 Quality of life At baseline 39.5±23.3 35.8±21.5 .46 At 90 days 27.4±21.7 27.3±21.6 .98 Caregiver mastery At baseline 24.7±3.3 26.3±3.7 .05 At 90 days 25.2±3.8 25.8±3.0 .38 Values are expressed as mean ± SD. Progress in Cardiovascular Nursing® (ISSN 0889-7204) is published Quarterly (March, June, Sept., Dec.) by Le Jacq, located at Three Enterprise Drive, Suite 401, Shelton, CT 06484. Le Jacq is an imprint of Blackwell Publishing, which was acquired by John Wiley & Sons in February 2007. Blackwell’s programme has been merged with Wiley’s global Scientific, Technical, and Medical business to form Wiley-Blackwell. Copyright ©2008 by Le Jacq. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or
- 35. any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Ben Harkinson at [email protected] or 781-388-8511. ® Winter 2008 Progress in Cardiovascular Nursing 25 time should also be considered. Future research is needed to learn more about EHM as a convenience to patients, especially those who are homebound, travel frequently, are socially isolated, have transportation costs associated with office visits, or work outside the home during typical physician office hours. Telemonitoring offers health care providers and patients interaction at a distance, when away from home, and at the convenience of both parties. Depressive symptoms and caregiver mastery have rarely been studied in patients receiving a home monitoring intervention. Depressive symptoms were low and caregiver mastery was high in both groups and did not differ significantly due to EHM. These find- ings concur with those of Friedman and Griffin38 who found that patients
- 36. were not generally depressed. Contrary to the findings of Benatar and col- leagues21 and Bondmass and cowork- ers,22 quality of life scores did not differ significantly between groups. Reasons for these findings may be related to the length of time that fam- ily members had been providing care and the type of care provided. Most patients in this sample had been living with HF or required assistance from a caregiver for an average of 4 years. Caregivers remarked that they had adjusted to the problems that accom- pany limited activity, many had very good insurance benefits from their past employers, and they expected the changes that come with aging. Informal social support was high in this sample and was not a sig- nificant predictor of risk of readmis- sion. Although Schwarz32 found that tangible social support predicted less early hospital readmission, the sample included patients with multiple comor- bidities in addition to HF and who were more functionally impaired. Limitations Our study has several limitations. Our findings are limited to patients classified in NYHA classes II, III, and IV. Since 31% of patients in this study were NYHA class IV, a replication study
- 37. using less severely ill patients may lead to greater differences between groups, even with a short follow-up period. Although the majority of intervention patients reported that they used the EHM system on a regular basis, the PI did not have information about whether teaching before hospital discharge was consistent between groups. Functional status, number of comorbidities, and medication use did not differ significantly between groups at baseline or 90 days’ postdis- charge. Patients subjectively reported their functional abilities, however, and severity of comorbidities was not stud- ied. In past studies of patients with HF, researchers reported variations in how medications were prescribed and issues with compliance.39,40 Although patients reported taking medications as prescribed, a formalized monitor- ing system was not used. Information about dosages or changes in medica- tions was not collected, and these variables could have differed between groups and affected results. Specific number of visits to the patients’ cardiologist/primary physi- cian and how physicians responded to nursing assessments were also not obtained as part of the study. Several of the cardiologists voiced concerns about the amount of paperwork involved
- 38. when monitoring via an EHM system. Lack of attention to paperwork could have minimized information used in decision making and therefore limited actions that could have prevented hos- pitalization or early readmission. Limitations of the study may be due to absence of control over usual care provided by the home care agen- cy. Contrary to this study, others used a study nurse to provide care, and together the PI and nurse reviewed assessments of patients.20 Finally, there was no group that received EHM and not home care in our study. Thus, we do not know whether EHM would benefit patients who have a similar status as a solo resource/service. CONCLUSIONS Telemonitoring by EHM did not reduce rates of hospitalization, emergency department visits, cost of care, or depression, and it did not increase caregiver mastery, quality of life, or days to readmission; however, EHM did not cause harm, as there were no negative differences between groups in primary outcomes. Further EHM technological developments may enhance self-management of HF and eventually lead to improved clinical outcomes. Research is needed to better target those most likely to
- 39. benefit from this intervention. Future research should address the interaction between the APN and follow-up intervention with telemonitoring. Disclosure: The project was supported by Grant Number 1 R15 R008698–01 from the National Institute of Nursing Research, National Institutes of Health (NIH), and the Ohio Board of Regents. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the National Institute of Nursing Research, NIH. REFERENCES 1 Rosamond W, Flegal K, Friday G, et al, on behalf of the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2007;115:e69–e171. 2 Rich MW. Heart failure disease management: a critical review. J Card Fail. 1999;5:64–75. 3 Proctor EK, Morrow-Howell N, Li H, et al. Adequacy of home care and hospital readmis- sion for elderly congestive heart failure patients. Health Soc Work. 2000;25:87–94. 4 Naylor MD, Brooten D, Campbell R, et al. Comprehensive discharge planning and home follow-up of hospitalized elders: a randomized
- 40. clinical trial. JAMA. 1999;281:613–620. 5 Anderson MA, Clarke MM, Helms LB, et al. Hospital readmission from home health care before and after prospective payment. J Nurs Scholarsh. 2005;37:73–79. 6 Casper GR, Kenron DA. A framework for tech- nology assessment: approaches for the selection of a home technology device. Clin Nurse Spec. 2005;19:170–174. 7 Jiang W, Alexander J, Christopher E. Relationship of depression to increased risk of mortality and rehospitalization in patients with congestive heart failure. Arch Intern Med. 2001;161:1849–1856. 8 Vaccarino V, Stanislav VK, Abramson J, et al. Progress in Cardiovascular Nursing® (ISSN 0889-7204) is published Quarterly (March, June, Sept., Dec.) by Le Jacq, located at Three Enterprise Drive, Suite 401, Shelton, CT 06484. Le Jacq is an imprint of Blackwell Publishing, which was acquired by John Wiley & Sons in February 2007. Blackwell’s programme has been merged with Wiley’s global Scientific, Technical, and Medical business to form Wiley-Blackwell. Copyright ©2008 by Le Jacq. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily
- 41. reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Ben Harkinson at [email protected] or 781-388-8511. ® Progress in Cardiovascular Nursing Winter 200826 Depressive symptoms and risk of functional decline and death in patients with heart failure. J Am Coll Cardiol. 2001;38:199–205. 9 Oxman TE, Hull JG. Social support and treatment response in older depressed primary care patients. J Gerontol B Psychol Sci Soc Sci. 2001;56:P35–P45. 10 National Academy on Aging Society. Heart disease: a disabling yet preventable condition. http://www.agingsociety.org/agingsociety/pdf/ heart.pdf. Accessed May 1, 2000. 11 Rector TS, Kubo SH, Cohn JN. Patient’s self- assessment of their congestive heart failure: part 2. Content, reliability, and validity of a new measure, the Minnesota living with heart failure questionnaire. Heart Failure. 1993;3:198–209. 12 Pugh LC, Havens DS, Xie S, et al. Case manage- ment for elderly persons with heart failure: the quality of life and cost outcomes. Medsurg Nurs. 2001;10:71–84. 13 Goldberg LR, Piette JD, Walsh MN, et al. Randomized trial of a daily electronic home
- 42. monitoring system in patients with advanced heart failure: the Weight Monitoring in Heart Failure (WHARF) trial. Am Heart J. 2003;146:705–712. 14 Pearlin LI, Mullan JT, Semple SJ, et al. Caregiving and the stress process: an overview of the concepts and their measures. Gerontologist. 1990;30:583–591. 15 Scott LD. Technological caregiving: a qualitative perspective. Home Health Care Manage Pract. 2001;13:227–235. 16 Schwarz KA. Home health care: formal social support to family caregivers of older adults. Family Perspective. 1996;30:47–61. 17 Schwarz KA, Elman C. Identification of factors predictive of hospital readmissions for patients with heart failure. Heart Lung. 2003;32:88–99. 18 Stewart S, Marley JE, Horowitz JD. The addition of a home visit by a cardiac nurse to usual multi- disciplinary care reduced deaths and readmissions in patients with chronic congestive heart failure. Lancet. 1999;354:1077–1083. 19 Rich MW, Beckham V, Wittenberg C, et al. A multidiscliplinary intervention to prevent the read- mission of elderly patients with congestive heart failure. N Engl J Med. 1995;333:1190–1195. 20 Jerant AF, Azari R, Nesbitt TS. Reducing the cost of frequent hospital admissions for congestive heart failure: a randomized trial of a home telecare
- 43. intervention. Med Care. 2001;39:1234–1245. 21 Benatar D, Bondmass M, Ghitelman J, et al. Outcomes of chronic heart failure. Arch Intern Med. 2003;163:347–352. 22 Bondmass M, Bolger N, Castro G, et al. The effect of physiologic home monitoring and telemanagement on chronic heart failure out- comes. Internet J Asthma Allergy, Immunol [serial online]. http://www.ispub.com/ostia/index. php?xmlFilePath=journals/ijanp/vol3n2/chf.xml. Accessed April 30, 2002. 23 Roglieri JL, Futterman R, McDonough KL, et al. Disease management interventions to improve outcomes in congestive heart failure. Am J Manag Care. 1997;3:1831–1839. 24 McManus SG. A telehealth program to reduce readmission rates among heart failure patients: one agency’s experience. Home Health Care Manage Pract. 2004;16:250–254. 25 Hunt SA, Abraham WT, Chin MH, et al, on behalf of the American College of Cardiology, the American Heart Association Task Force on Practice Guidelines, the American College of Chest Physicians, the International Society for Heart and Lung Transplantation, and the Heart Rhythm Society. ACC/AHA guideline update for the diagnosis and management of chronic heart failure in the adult: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001
- 44. Guidelines for the Evaluation and Management of Heart Failure): developed in collaboration with the American College of Chest Physicians and the International Society for Heart and Lung Transplantation: endorsed by the Heart Rhythm Society. Circulation. 2005;112:e154–e235. 26 Bennett JA, Riegel B, Bittner V, et al. Validity and reliability of the NYHA classes for measur- ing research outcomes in patients with cardiac disease. Heart Lung. 2002;31:262–270. 27 Katz S. Assessing self-maintenance: activi- ties of daily living, mobility, and instrumen- tal activities of daily living. J Am Geriatr Soc. 1983;31:721–726. 28 Lockery SA, Dunkle RE, Kart CS, et al. Factors contributing to the early rehospitalization of elder- ly people. Health Soc Work. 1994;19:182–191. 29 Lawton MP, Brody EM. Assessment of older peo- ple: self-maintaining and instrumental activities of daily living. Gerontologist. 1969;9:179–186. 30 Spector WD, Fleishman JA. Combining activities of daily living with instrumental activities of daily living to measure functional disability. J Gerontol B Psychol Sci Soc Sci. 1998;53:S46–S57. 31 Radloff LS. The CES-D scale. A self-report depression scale for research in the general popu- lation. Appl Psychol Meas. 1977;1:385–401. 32 Schwarz KA. Predictors of early hospital read- missions of older adults who are functionally
- 45. impaired. J Gerontol Nurs. 2000;26:29–36. 33 Rector TS, Cohn JN. Assessment of patient outcome with the Minnesota living with heart failure questionnaire: reliability and valid- ity during a randomized, double-blind, placebo- controlled trial of pimobendan. Am Heart J. 1992;124:1017–1025. 34 Lawton MP, Kleban MH, Moss M, et al. Measuring caregiver appraisal. J Gerontol. 1989;44:P61–P71. 35 Sevick MA, Matthews JT, Wielobob C, et al. Volume-based ventilator-dependent patients: measurement of the emotional aspects of home caregiving. Heart Lung. 1994;23:269–278. 36 Krause N, Markides K. Measuring social sup- port among older adults. Int J Aging Hum Dev. 1990;30:37–53. 37 Allison PD. Survival Analysis Using the SAS System: A Practical Guide. Cary, NC: SAS Institute; 1995. 38 Friedman MM, Griffin JA. Relationship of physi- cal symptoms and physical functioning to depres- sion in patients with heart failure. Heart Lung. 2001;30:98–104. 39 De Geest S, Scheurweghs L, Reynders I, et al. Differences in psychosocial and behavioral pro- files between heart failure patients admitted to cardiology and geriatric wards. Eur J Heart Fail. 2003;5:557–567.
- 46. 40 Bennett SJ, Huster GA, Baker SL, et al. Characterization of the precipitants of hospital- ization for heart failure decompensation. Am J Crit Care. 1998;7(3):168–174. Progress in Cardiovascular Nursing® (ISSN 0889-7204) is published Quarterly (March, June, Sept., Dec.) by Le Jacq, located at Three Enterprise Drive, Suite 401, Shelton, CT 06484. Le Jacq is an imprint of Blackwell Publishing, which was acquired by John Wiley & Sons in February 2007. Blackwell’s programme has been merged with Wiley’s global Scientific, Technical, and Medical business to form Wiley-Blackwell. Copyright ©2008 by Le Jacq. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Ben Harkinson at [email protected] or 781-388-8511. ® Since I’ve been teaching this course, I’ve learned that a lot of students have difficulty with this assignment. Here is some guidance that might help you complete this assignment successfully. The numbers pertain to the question number. 1. The purpose of the study is clearly and explicitly stated in this article.
- 47. 2. The research question is clearly and explicitly stated in this article. 3. Go back to Week 3 lesson and to chapter 2 of your text to review research designs. This article explicitly states the research design. 4. The question specifically states to go to Chapter 2 in your text and look at the qualitative characteristic in the table (2.1). Using this table, identify any of those characteristics that this study contains. 5. Make sure you go to the journal’s (not the article) website. It answers this question. Just Google the name of the journal and you should find the website. You can also find a checklist to determine if a source is credible (including evidence of peer review) in your text. 6 and 7 are pretty self-explanatory. 8. Identify the TYPE of sampling that was used and the strengths and weaknesses of this type of sampling. Go back to Week 4 lesson and chapter 7 in your text. Identify the criteria used for inclusion in the study 9. Go to your text to see the definition of vulnerable populations. 10. Self-explanatory The second article is more difficult, I think. 11. The purpose of the study is clearly and explicitly stated in this article. 12. The questions are explicit in this article, but they are called “hypotheses”. 13. The authors did not fully describe the design of the study,
- 48. but do talk about setting, sample, and what and how statistics were collected – this will enable you to deduce the design of the study. 14. Go back to Chapter 2 of your text again and do the same thing you did for question 4. 15. See #5. 16. Self explanatory. 17. The population of the study is clearly and explicitly stated in this article. 18. See question 8 19. See question 9 20. Self explanatory. Telemonitoring of heart failure patients and their caregivers: a pilot rand... Basic Search Advanced Publications Browse Preferences English Help Full text
- 49. Full Text A Process of Decision Making by Caregivers of Family Members With Heart Failure Sanford, Julie, DNS, RN; Townsend-Rocchicciolli, Judith, PhD, RN; Horigan, Annie, MSN, RN; Hall, Pat, PhD, CRNP. Research and Theory for Nursing Practice 25.1 (2011): 55-70. Abstract (summary) Heart failure (HF) is a major cardiovascular problem and the number of people living with HF continues to climb. Throughout the illness continuum, patients and their family caregivers are involved in decision making. As the illness worsens and patients can no longer make decisions, decision making becomes the responsibility of their caregivers who may have little preparation for the role. The purpose of this grounded theory study was to examine how caregivers of family members with HF make decisions. A nonlinear decision- making process consisting of several actions was identified, which included actualizing; seeking input, information, or support; reflecting; choosing; evaluating; and validating the decision. Headnote Heart failure (HF) is a major cardiovascular problem and the number of people living with HF continues to climb. Throughout the illness continuum, patients and their family caregivers are involved in decision making. As the illness worsens and patients can no longer make decisions, decision making becomes the responsibility of their caregivers who may have little preparation for the role. The purpose of this grounded theory study was to examine how caregivers of
- 50. family members with HF make decisions. A nonlinear decision- making process consisting of several actions was identified, which included actualizing; seeking input, information, or support; reflecting; choosing; evaluating; and validating the decision. Keywords: decision making; heart failure; caregiving; grounded theory Heart failure (HF), a complex cardiovascular syndrome, is increasing in incidence throughout the world. In 2003, the World Health Organization (WHO) noted that cardiovascular disease accounted for more than 16.7 million deaths (29.2%) of all deaths worldwide with 7.2 million of these deaths attributed to ischemic heart disease. According to the American Heart Association (AHA), almost 6 million Americans have HF with more than 670,000 new patients who are 45 years of age or older diagnosed each year (AHA, 2009). In 2003, the Study Group on HF Awareness and Perception in Europe (SHAPE) noted that approximately 14 million people in Europe currently suffer from HF and suggests that number will escalate to more than 30 million Europeans by the year 2020 as the population ages. Blackledge, Tomlinson, and Squire (2003) predict that nearly 40% of HF patients will die within 1 year of hospitalization as case fatality remains high and prognosis poor. As the global population ages, the economic impact of HF on global health systems will become even greater. Historically, patients with HF faced rapid deterioration and quickly died from the disease. With advances in pharmacologic therapy and other treatment interventions to support the failing heart, the trajectory of illness in HF has evolved into one that is more
- 51. gradual in its progression, allowing patients to live longer, lead more productive lives, and make more decisions as their health status changes. When the patient with HF is discharged from the acute care facility or rehabilitation center, the family may become overwhelmed with the physical and mental requirements of care and the many decisions that must be made. Family caregivers of patients with HF often do not possess the skills necessary to navigate health care systems that have become increasingly complex. Implicit in this need to make decisions is the ability of the caregiver to make treatment decisions or assist with decision making at critical points as the disease progresses. The family's ability to cope effectively and make good treatment decisions with the needs of the patient in mind may affect the patient's outcome (Family Caregiver Alliance, 2009). To assist patients with HF and their caregivers in making treatment and care decisions, nurses must understand how the decision process for caregivers occurs. Caregivers have an integral and critical role throughout the illness experience and play a crucial part in the decision- making process; however, little is known about how they make decisions for patients with HF. The purpose of this study is to describe decision making by caregivers of patients with HF. The specific research question for this study is this: How do caregivers of family members with HF make decisions? CAREGIVING AND DECISION MAKING Caring for a patient with HF is stressful and becomes more so as the disease progresses and physical and emotional care become more difficult. The need
- 52. for complex decision making becomes apparent. Estimates of the numbers of family caregivers in the United States vary based on the definitions and criteria used. A 2004 report estimates that 22.9 million households or 44.4 million Americans are involved in caring for a person aged 50 and older (National Alliance for Caregiving and the American Association for Retired Persons, 2004). Rogers and Komisar (2003) report that 13 million adults in the United States have chronic conditions that impair their ability to function independently. Although there are no exact numbers of informal caregivers of patients with HF, it is clear that the projected numbers will increase as the disease incidence increases in an aging society. http://search.proquest.com.proxy.devry.edu/?accountid=147674 http://search.proquest.com.proxy.devry.edu/advanced?accountid =147674 http://search.proquest.com.proxy.devry.edu/docview.pagelayout :publication?t:ac=853503862/Record/354CEF3F10A4D9CPQ/6 http://search.proquest.com.proxy.devry.edu/docview.pagelayout :browse?t:ac=853503862/Record/354CEF3F10A4D9CPQ/6 http://search.proquest.com.proxy.devry.edu/docview/853503862 /354CEF3F10A4D9CPQ/6?accountid=147674# http://search.proquest.com.proxy.devry.edu/docview/853503862 /354CEF3F10A4D9CPQ/6?accountid=147674# javascript:newPopup('/help/academic/webframe.html?Document _overview.html'); http://www.springerpub.com/ http://search.proquest.com.proxy.devry.edu/indexinglinkhandler /sng/au/Sanford,+Julie,+DNS,+RN/$N?accountid=147674 http://search.proquest.com.proxy.devry.edu/indexinglinkhandler /sng/au/Townsend- Rocchicciolli,+Judith,+PhD,+RN/$N?accountid=147674 http://search.proquest.com.proxy.devry.edu/indexinglinkhandler /sng/au/Horigan,+Annie,+MSN,+RN/$N?accountid=147674
- 53. http://search.proquest.com.proxy.devry.edu/indexinglinkhandler /sng/au/Hall,+Pat,+PhD,+CRNP/$N?accountid=147674 http://search.proquest.com.proxy.devry.edu/pubidlinkhandler/sn g/pubtitle/Research+and+Theory+for+Nursing+Practice/$N/288 49/DocView/853503862/fulltext/$B/1?accountid=147674 http://search.proquest.com.proxy.devry.edu/indexingvolumeissu elinkhandler/28849/Research+and+Theory+for+Nursing+Practic e/02011Y04Y01$232011$3b++Vol.+25+$281$29/25/1?accounti d=147674 The daily continuing burden of caregiving can result in negative physical, mental, emotional, and social outcomes (Family Caregiver Alliance, 2009). Luttik, Jaarsman, Veeger, and Van Veldhuisen (2005) note the burden caregivers encounter when caring for patients with HF, suggesting that oftentimes, the caregivers have greater physical challenges than the patient. Caregivers have little preparation for the caregiving role and are in great need of physical, emotional, and respite support as well as support to make sound decisions. Decision Making in Caregiving With advances in medicine, people with chronic illnesses are living longer, many times necessitating assistance with or abdication of the decision making to their caregivers. As the patient's health declines, caregivers are called on to make decisions more frequently (Hall, Sanford & Demi, 2008). Although the patient may have discussed their wishes or left written documentation of their preferences for care, such requests often do not have an impact on the decisions that are eventually made by caregivers (Shalowitz, Garrett-Mayer, & Wendler, 2006; Vig, Taylor, Starks, Hopley,
- 54. & Fryer-Edwards, 2006). An understanding of how caregivers make decisions can serve to strengthen needed support and information during the caregiving experience. Caregivers affect how decisions concerning the health of the patient occur, particularly when the patient can no longer make decisions on their own. It is important to note that decision-making studies are more prevalent in other chronic diseases such as cancer, dementia, and renal failure, but few studies are available that examine decision making in HF. This is significant in that caregivers' decisions may ultimately affect the entire family and may create strain on the patient and caregivers themselves. It is often hard to separate what is best for the patient and what is best for the family. A major challenge that caregivers face is making decisions for a family member who has impaired judgment (Menne & Whitlatch, 2007). Empirical Evidence Regarding Caregiver Decision Making. Research has shown that shared decision making between patient with HF and the caregiver can lead to a better self-care. Sebern and Riegel (2009) found that older patients with HF and caregivers who report their patient's health as good also report better shared communication and decision making, self-care maintenance, and self-care confidence. However, not all caregivers and patients want information regarding the prognosis of the illness. Fried, Bradley, and O'Leary (2003) studied end-of-life care in cancer patients and found that many elders and caregivers are unable or unwilling to accept a prognosis of limited life expectancy despite previous reports indicating a desire for such disclosure. Hansen, Archbold, Stewart, Westfall, and Ganzini (2005) report
- 55. that role strain for caregivers exists during the actual decision- making phase, as well as during the days, months, and years prior to the event and may continue after the decisions are made. Quinn, Dunbar, and Higgins (2010) examined the degree of congruence between patients with HF and their primary caregivers on symptom assessment and self-care management behaviors. Findings suggest that caregiver as proxy appears to be a reasonable substitute for patient's responses in a community setting. The study is important in that it validates the importance of the need for caregivers to have specific knowledge of the disease to make the best decisions possible. Theoretical Evidence Regarding Caregiver Decision Making. Examining the evidence of how caregivers and patients with HF make decisions to engage in self-care is also an important consideration in how decision making occurs in HF. In a qualitative study, Clark et al. (2008) examined individual and contextual factors perceived by patients and their informal caregivers that influence their willingness to undertake effective HF self-care. This study is significant in that it suggests that knowledge of HF is potentially a determinant of outcomes based on the ability of the caregiver to make decisions. A grounded theory study by Crist, Garcia-Smith, and Phillips (2006) examined the process by which 23 Mexican American elders and their caregivers decided to use formal home care services. A three-stage theory emerged that describes the decision process to use formal home care: taking care of our own, acknowledging options, and becoming empowered. This study is important in caregiving decision research in that it purports that the Mexican American
- 56. family maintains their cultural norms while making difficult treatment decisions. In a phenomenological study in Taiwan, nine mothers shared their experience of family interactions and relationships while facing decisions about their child's heart surgery. A five-step decision process emerged and findings indicate the entire family experienced psychological distress, role reorganization, and a remodeling of family functioning (Shu-Fan, Pei-Fan, & Kai-Sheng, 2007). Hall et al. (2008) examined moral decision making by wives of patients with life-threatening cardiovascular disease. Using grounded theory, factors influencing decision making and decision-making patterns were identified. Hall (1994) describes a five-step process of decision making, which includes searching, seeking, reflecting, accepting, and decision making. This study was limited to only one specific group of caregivers and examined decision making retrospectively after a family member had died. Application of this theory to concurrent decision making by caregivers other than wives forms the foundation for the current study. After review of the literature and examination of possible theories that could explain how caregivers of family members with HF make decisions, researchers determined that none is sufficient to explain how this group makes decisions. As a result, these theories are used as a sensitizing framework for the current study. Although there is limited empirical evidence that validates how decision making occurs between patients with HF and their caregivers, it is clear that the willingness, knowledge, and ability to make these decisions is inherent in the outcomes of care.
- 57. METHODS A qualitative design using grounded theory methods was used to examine the process of decision making among caregivers of patients with HF (Charmaz, 2006). After Institutional Review Board approval, 20 participants were recruited from cardiology offices, inpatient hospital units, or adult day care facilities over a 12-month period from 2008-2009. To ensure data variation, five caregivers of patients with HF were interviewed from each of the four stages of the HF classification (Hunt et al., 2005). To qualify as a participant, the caregiver had to be related to the patient with HF, provide one activity of daily living, and/or assist the care recipient with two instrumental activities of daily living and not be paid for services. Demographic data collected included caregiver gender, marital status, ethnicity, employment status, income, living arrangement, and relationship to patient with HF. Data Collection After informed consent was obtained, unstructured open-ended interviews were conducted in private mutually agreed on locations: the caregivers' homes, places of employment, or the library. The interviews were audiotaped and questions began broadly with statements such as, "Tell me about your family member's illness." As the conversation progressed, questions specifically related to decision making were asked (see Table 1 for the interview guide). The interviewers kept memos about the experience and took notes on key points that needed further clarification. Interviews lasted from 45 minutes to 2 hours, which included time for completion of demographic data. The
- 58. sample includes 20 caregivers of family members of patients with HF who live in the Southeastern United States (see Table 2 for demographic characteristics of the participants). Data Analysis Data were transcribed verbatim, checked for accuracy, and entered into the NVivo qualitative software program. Researchers independently coded the data line by line after each interview and then met for focused coding to develop the most salient categories of the data. The core conceptual categories were identified, and links between them resulted in theoretical categories. As data were analyzed, theoretical sampling of pertinent data was used to elaborate and refine categories in the emerging theory until saturation was obtained (Charmaz, 2006). Memo writing of impressions during data collection, thoughts during analysis, and progression to theoretical development were completed to ensure rigor of the study. A theoretical model was developed that describes the process of decision making by caregivers of family members with HF (see Figure 1). Triangulation is a method used by qualitative researchers to establish validity in their work (Guion, 2002). Theory triangulation involves the use of multiple theoretical perspectives to draw inferences or conclusions from a set of data in an effort to validate data findings (Watson, McKenna, Cowman, & Keady, 2008). Theory triangulation was used to determine if the process of decision making among participants in this study is linked with a theory that emerged from a previous study of
- 59. decision making by wives of patients with HF at end of life (Hall, 1994), as well as comparing findings to current literature. FINDINGS The theoretical model (see Figure 1) that emerged from data describes the process of decision making by family caregivers of patients with HF. Generally, caregivers make decisions through a process of phases; though at any time, caregivers may progress through these actions in a nonlinear fashion. Phase 1: Actualization of Issue, Problem, or Challenge Caregivers of patients with HF are confronted with many types of decisions. Some decisions occur at the onset of diagnosis, whereas others, such as when to go to the hospital and decisions about whether to work, are revealed as the patient continues through the disease process. Actualization of an issue, problem, or challenge, the realization that the caregiver has a decision to make, seems to be especially pertinent at the point of diagnosis. A few caregivers note that their family member is dealing with what they thought to be stable chronic illnesses and the diagnosis of HF itself seems to blindside them. A 34- year-old African American wife of a patient with Stage II HF states, "A cardiologist came in and that was when, as we put it, 'all hell broke loose.' They told us that he was diagnosed with HF. So, there were no prior signs or any type of heart problems." Actualization of a problem is experienced as a change in how common decisions about everyday life are affected by illness. Decisions that used to be simple
- 60. and uncomplicated now have an additional layer of complexity due to the illness. A 26-year-old African American wife of a patient with Class III HF shares, "We have had to make decisions based on everything in our life. We can't even decide on a vacation without having considerations about his health and ability. How long we stay, where, what devices we need." Significant situations that emerge as challenges that caregivers have to make decisions about include when to access the emergency medical system, when to go to the doctor, and how to manage medication. Contemplating a situation when her husband's implanted defibrillator went off, a 42- year-old White caregiver of a patient with Stage III HF states, "Now if it had knocked him out cold, I wouldn't have hesitated. I would have automatically called 911. That was what helped me make that decision." Patients with HF who become symptomatic need adjustment of their medications that often require intervention by caregivers. One African American daughter who cared for her 76-year-old mother with Stage IV HF shares how she monitors her mother's blood pressure and adjusts medications as instructed, "From time to time, we change her medication, especially when its [BP] real abnormal." Another issue that requires decision making by almost all caregivers interviewed includes the need to make financial and work decisions. Caregivers often have to face the challenge that there is no other choice for their loved one but to seek disability. The inability to sustain employment is in stark contrast to their youth and the expected role of their family member and points to the seriousness of the diagnosis. A 34-year-old African American wife of a patient with Stage II HF stated, "The doctors came in to tell us
- 61. everything about filing for disability . . . doctors don't come and tell you at a young age when you're full of life to fill out disability papers because they don't want you on it." Phase 2: Seeking Information, Input, or Supp ort The next phase in the theoretical model that emerged from the data is seeking information, input, and support. Caregivers of patients with HF consistently share that they need to get information, input, and support for the decision to be made. Patient input is desired above all others in the caregivers' need to put the patient as the focus of the decision. Some caregivers share that the patient is still the primary decision maker although the caregiver often have great influence in the choice that is made. Patient abdication of decision making somewhat correlates with the trajectory of illness; other times it is dependent on the relationship between the patient and caregiver. As caregivers assume more of the responsibility for decision making, they are clear in their need for information, input, and support from others. A 49-year-old White caregiver of her spouse, who has Stage II HF, states, Currently he is still making the majority [of decisions] but he isn't making them alone. He knows what he wants but he doesn't know how to get it or he doesn't have the patience. So he comes to me, we research it together, we talk about the decisions that need to be made, and I talk him into what he needs to do. Caregivers sought to include others when making decisions and sought support and input from many sources. A caregiver who
- 62. depends on support from others for decision making states, "I wouldn't suggest that anybody try to do it (make decisions) by themselves. It would tear you apart." Information is critical to the caregivers' ability to make decisions, whether that choice is made with the patient or for the patient. A 51-year-old White wife whose husband suffers from Stage III HF shares, "Now as far as how we make decisions, information is very important to us, we have to have a lot of information, medically to look at pros and cons." Another caregiver, a 36-year-old African American whose mother has Stage IV HF shares, "Yeah, I'm a hairdresser so I deal with a lot of people with HF, high blood pressure, all of these conditions . . . talking to the customers you know I learned . . . really talking with people and getting information." Caregivers often share that the process of seeking information occurs simultaneously with seeking input and support. A 38- year-old African American wife of a patient with Stage III HF states, "Everybody has health issues and they kinda bounce them off of each other. They are supportive. They are in contact a lot." And, We always talk to our extended family, our parents, my sister . . . friends give us advice and guidance and support in difficult times as well as difficult decisions . . . We have been very much together and a partnership. John knows everything about his condition, there are no secrets and we both want
- 63. honest evaluation and appraisals so we can make decisions. Caregivers are clear that support is necessary for good decision making. They share that family, friends, and health care providers are essential sources of support and information. A 49-year-old White caregiver whose husband has Stage III HF states, "You need someone that can support you . . . someone that can be there . . . it is like you are the go to person and you need someone to go to and if nobody is there, that is hard." Caregivers share that relationships with health care providers are essential because they provide support and understanding that is critical to the decision making process. A 56-year-old White caregiver whose husband has Stage II HF shares, "I have visited doctors who were in and out [of the examination room]. But the people that we have met have told us what they thought, and how they intended to work with us and deal with it." Health care providers who view the caregiver as a partner in the treatment plan of the patient with HF provide support and understanding that caregiver's state is critical to the decision- making process. An African American caregiver whose 43-year-old husband has been recently diagnosed with Stage III HF shares, The nurse called after he had an echo done. She said, "Well, he is going to have to have a pacemaker. How would you like to do this, would you like to tell him first, and then he come in and talk to the doctor, or would you rather the doctor told him?" I will be forever grateful for that, just for her to give me the opportunity to sit down and initially break it to him. Caregivers also share that they need to seek spiritual support when caring and making decisions for their family members
- 64. with HF. A 55-year-old White caregiver whose mother has Stage II HF states, "If nothing else, find you a church and realize that you can't make someone do something and you just have to accept what changes they are willing to make." A 43- year-old African American whose mother has Stage IV HF states, "All you can do is hope and pray that you make the right decisions, stay strong and give it your all and try your best and take one day at a time. Phase 3: Reflecting For the caregivers of patients with HF, the ability to manage what is often complex and unfamiliar information they receive from physicians, nurses, friends, and family is frequently frightening and involves a period of thinking and self-reflecting prior to making a decision. As the concept of reflection emerges in the model, it is often employed as a means for review of how information is received and handled. Reflection is spontaneous in nature and allows caregivers to assess information, examine their problem-solving ability, and put their thoughts into an organized perspective. In addition, reflecting via discussion with others often illustrates selfawareness of an issue as well as insight into a specific behavior or a "why" something is done. One 49-year-old White caregiver, when reflecting on how she uses information to make decisions about her husband with Stage III HF says, "I guess the best way I make decisions is try to look at the big picture and long-term effects versus what it's like right now. I can't afford to not sit down and rationally think something out." Phase 4: Decision Choice
- 65. After realizing that they are faced with an issue or challenge, seeking input or support, and reflecting on their options, it becomes apparent that about midway through this process, caregivers have to make a decision or a choice. One caregiver recalls how she has to make choices about her husband's health even though her husband with Stage II HF may feel she is overreacting. The 42-year-old White caregiver shares, "I wanted to call 911 but he is hardheaded and it is hard for me to do it because if he doesn't want me to, it stresses him out even more. Sometimes I have to go over his head." Phase 5: Evaluating Decision Choice Once a decision is made, caregivers critically evaluate that choice to determine if the right decision has been made. A 24- year-old African American caregiver who makes difficult treatment decisions for her husband diagnosed with Stage IV HF evaluates her decision choice when she shares, "That was hard, it has really taught me to be a little bit more adult like in my decisions. I had to figure out if I had done the right thing." Whether the decisions relate to managing medications, decisions about family and work, or disease treatment, caregivers evaluate the decisions they make. A 44-year-old daughter who provides care for her father with Stage III HF refers to how she evaluates her decision choice, "Just going with your gut feeling and trying to make sure you make the best choice. I don't care if it causes conflict. I'll just make the decision, think about it, and be confident in the decisions I make." Phase 6: Seeking Validation
- 66. Seeking validation occurs at each phase of the decision-making process of the caregivers. Validating emerges as an important task for caregivers, particularly in the areas of seeking information and input, and decision choice. Some caregivers seem to second-guess their decisions, but most caregivers make decisions and move forward. Researchers note that caregivers ask questions and validate information with physicians and nurses at many points along the disease trajectory. Family also assists with validating decisions. A White 48-year-old daughter who provides care for her mother with Stage II HF reports validating information with her aunt, and although her aunt did not assist in any actual decision making, she serves as a sounding board, which allows the caregiver to stay focused and on track. Influences and Context The process of decision making is influenced by situations, people, relationships, and the environment. As the caregivers describe how they make decisions, they also share what influences their decision making. In the background of the decisionmaking process is the context of the caregiver and patient. Context is the world the family lives in, and how their world influences decision making is unique for each family. Several themes emerge from the data regarding influences and context that are shared by most caregivers. The relationship between caregivers and their family member is an essential influence on the decision-making process. A 34- year-old African American married participant expresses the shock at having to adjust her expectations to this life-threatening disease when she states,
- 67. I think we are at a very young age to have to be making these decisions. We have had a lot of crises since we have been married. This is not the Cinderella- type marriage I thought I would have. These are not the decisions I thought I would be making for my husband at age 40. Another wife, a 52-year-old White woman, shares that her relationship with her husband who has Stage II HF has caused them both to grow, stating, "I feel very positive that we have the kind of relationship we do where we talk about these things together and listen to others' advice." Each caregiver identifies family relationships as significantly influencing decision making. Strong relationships with family members are consistently cited as a positive influence, whereas difficult family relationships often lead to stress for the caregiver and patient with HF. Sibling relationships are frequently cited as influential to decision making. A 47-year-old White daughter, when discussing her sibling, shares, "There were times I needed help and I needed to work- she just couldn't do it. I told her right then, 'Well, you don't ever come up here and run the show when you can't show up now.'" An African American wife, 26 years old, whose husband is newly diagnosed with Stage III HF has to interact with skeptical in-laws stating, "My in-laws have his best interest at heart; this was like a deal breaker-type of situation. All eyes on me, 'Is she going to stick in there? Is she going to hang on?'" Relationships with children in the caregiver families also influence the decisions that are made. A 36-year-old White mother who cares for her husband with Stage
- 68. III HF and her 11-year-old son says, "My love for him [son] influences the decisions I make because he needs his Daddy." When making decisions for patients with HF, caregivers often express that their feelings and those of the patients' influence the process. Caregivers share that they are scared when making decisions. A 43-year-old White wife of a patient with Stage IV HF describes her fear of making the wrong decision, "I want to make the right decisions for him. I was scared of upsetting him more and him freaking out even more than he was already." Caregivers report that communication and relationships with health care providers also influence decision making. A 43-year-old White wife of a Stage III HF patient shares, "Communication with the health care workers dealing with my husband helps me make decisions." Consistently, one of the common themes that emerge as an influence to decision making is the financial considerations of the family. Families struggle with situations where patients with HF who are in their prime working years are suddenly diagnosed and could no longer earn an income. Caregivers also share their frustrations with the social security disability process and the length of time it takes to get a disability designation. These same caregivers share that they have difficulties working because they are afraid to leave their family members home alone or they have frequent absences to take their family members to appointments. Many patients who became unemployed have worked jobs that did not offer health insurance benefits and the financial toll on the family results in bankruptcy or severe financial strain. Caregivers spoke of the costs of medication and how they make
- 69. decisions about treatment regimens based on available resources for medication purchase. Those caregivers and patients who have health insurance express gratitude for the coverage. A 36-year-old African American wife of a patient with Stage IV HF describes viewing her husband's first hospitalization bill when he was diagnosed with HF: When I opened up that, I was like, I've got to be reading this wrong. I looked at it again and I saw $114,000. I saw six figures and tears began to roll down my face, and I really became emotional because all I kept thinking was, "God what if I didn't have this insurance?" Because at one point, he was in-between insurance and that October prior to him becoming sick, I transferred him on to my insurance. Though caregivers who have insurance are thankful, they still struggle with co-pays for medication, doctor visits, and hospitalizations. Caregivers share that the costs of medications to manage HF are expensive and that samples from the physician's offices often keep the patients from not doing without their medications. A 43-yearold White wife describes her husband's decision to not refill his carvedilol (Coreg), "He was off of it and I had no idea. He was out of it and even with my $50 co-pay, he couldn't pay it, and he didn't want to tell me. I said, 'That's your life or death.'" CONCLUSIONS Findings from this study highlight that the essence of decision making by caregivers of family members with HF is a nonlinear process consisting of several phases including actualization of the challenge, issue, or
- 70. problem; seeking input, information, or support; reflecting on the decision; making a decision choice; evaluating the decision made; and validating the decision. This study supports and validates findings from previous studies (Crist et al., 2006; Hall et al., 2008; Limerick, 2007; Shu-Fan et al., 2007) and expands understanding of the difficulties family caregivers of patients with HF encounter in making decisions. This study suggests that each action represents an important part of the process used by caregivers as they make decisions for their family member with HF. Actualizing the decision occurs when caregivers realize that a decision needs to be made on behalf of their family member with HF. Many different types of decisions are made, including those regarding medications, treatment procedures, finances, and range from simple to complex. Seeking information, primarily from health care providers, is considered by caregivers as essential to making decisions. Although caregivers consider their family members with HF to be the primary decision maker, when they are unable to do so or if the family member abdicates the decision making to the caregiver, the family member's input is considered most important. After caregivers gather information and receive input and support from others, a period of conscious reflection on their options for decision making occurs. Decisions that caregivers are presented with are often considered complex and frightening. At times, caregivers feel overwhelmed with their responsibility for decision making. Reflecting allows a time for caregivers to organize their thoughts and carefully consider all alternatives to avoid making ill-informed
- 71. decisions that may result in unwanted consequences, which may be regretted later. Understanding the possible choices, coming to terms with the need to act, and then choosing the best option from available alternatives enable caregivers to make a decision for their family member. Although caregivers frequently experience some relief in actually making the decision, they experience many other emotional reactions they then have to deal with. On occasion, when one decision is made, others emerge and caregivers have to start the whole process over with each new decision. Simultaneous decision making is not uncommon. Making the right decision is important to caregivers, and after arriving at a decision, they evaluate the decision to make sure they have made the right one. Seeking input and support from others as a means of validating that they made the right choice from available alternatives is important at this stage as well. Although most decisions are then implemented, sometimes alternatives present themselves, which result in making a different choice or returning to previous phases, especially seeking information and reflecting prior to making the decision. In addition, guessing their decision is not uncommon, and validation serves to confirm for caregivers that they made the right decision. Decision making does not occur in a vacuum and, in the case of decision making by caregivers of family members with HF, the context in which the decisions are made is an important consideration. Different
- 72. decisions are made at various points in time along the illness continuum. There are other factors that influence decision making such as the specific circumstances and situations when the decisions are made, individuals involved in the decision making and their relationship to one another, and the environment where the decisions are made. The most important variable affecting decision making is the relationship between caregivers and their family member. Health care providers play a pivotal role in assisting caregivers in making decisions by providing information as well as support. Caregivers consistently express concern for finances, which not only affect the decisions that are made but frequently add to the stress that caregivers experience. Few studies have examined the decision-making process used by caregivers of family members with HF; therefore, findings from this study are compared with those of prior studies that investigate caregivers' process of decision making. Findings from this study are similar to those described by Hall (1994); however, the current study further expands understanding of the process of decision making as well as specific factors affecting the decision-making process and the context in which it occurs for caregivers of family members with HF. Although the five-part decisionmaking model by Hall is validated in the current study, findings suggest that there are additional actions involved in the decision-making process such as actualizing the decision when caregivers are confronted with a decision to be made as well as evaluating and validating the decision choices. The previously described study by Crist et al. (2006) that examines the process by which Mexican American elders and
- 73. their caregivers decide to use formal home care services has commonalities with the current study. Their stage of acknowledging options is similar to the stage of actualizing in the current study and likewise requires seeking input, information, or support for the decision. What they describe as the process of becoming empowered actually occurs for participants in the current study during the time when they are validating the decision. Parallels can be drawn between findings from Shu-Fan et al. (2007) and the current study. Families in the Shu-Fan et al. study are shocked and confused when they learn of the child's diagnosis of a potentially lethal condition. Families transition through the hope that surgery would not be necessary but concluded that it is essential for the survival of their child. This step in the process is similar to that of actualization in the current study that caregivers realize there is a decision that must be made for the health of their loved one. Families also endeavor to make the right decision for their child, develop a trust for health care providers, and seek support from others who have gone through the same experience. Caregivers of those with HF consistently state that they need information and support from others to make the right decision for their family member. Further, they spend time evaluating their decision choice to ascertain whether the right decision has been made. Studies that explore caregivers' decision-making process regarding the withdrawal of life-sustaining treatments also support the current findings. Limerick (2007) found that there are three influencing domains that caregivers fluctuate among when making end-of-life decisions for their loved ones. Just as participants in the current study seek information, input, and