
Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to DIABETIC FOOT CASE PRESENTATION.pdf
Similar to DIABETIC FOOT CASE PRESENTATION.pdf (20)
More from varshawadnere
More from varshawadnere (20)
Recently uploaded
Recently uploaded (20)
DIABETIC FOOT CASE PRESENTATION.pdf
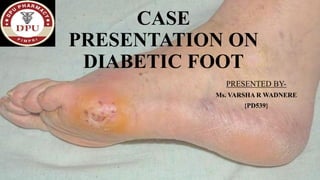
- 1. CASE PRESENTATION ON DIABETIC FOOT PRESENTED BY- Ms. VARSHA R WADNERE {PD539}
- 2. INTRODUCTION- DEFINITION Diabetic foot is one of the most significant and devastating complications of diabetes, and is defined as a foot affected by ulceration that is associated with neuropathy and/or peripheral arterial disease of the lower limb in a patient with diabetes. TYPES Diabetic foot is classified into two major types. • The Neuropathic Foot where neuropathy dominates • The Neuroischemic Foot, where occlusive vascular disease is the main factor, although neuropathy is present.
- 3. Wound classification system- Stages Description Stage A No infection or ischemia Stage B Infection present Stage C Ischemia present Stage D Infection and ischemia present Grading Grade 0 Epithelialized wound Grade 1 Superficial wound Grade 2 Wound penetrates to tendon or capsule Grade 3 Wound penetrates to bone or joint
- 4. RISK FACTORS • Age ≥ 45 years • Male gender • Charcot joint • Peripheral vascular disease • Peripheral neuropathy • DM Duration ≥10 years • Insulin use • Retinopathy • Nephropathy • Poor glycemic control • Cerebral vascular disease • Coronary heart disease • Hypertension • Smoking
- 6. TREATMENT GOALS 1. Eradication of clinical evidence of infection. 2. Avoidance of soft tissue loss and amputations. 3. Leg Conservation. 4. Rehabilitation of Patients. 5. Treatment and healing of DIABETIC FOOT. 6. Prevention of recurrence of DIABETIC FOOT and wounds. 7. Reduction of morbidity and mortality due to LEG.
- 7. DIAGNOSIS
- 8. SIGNS AND SYMPTOMS • Pain, erythema, and edema may be absent due to neuropathy • Pus • Delayed healing • Increased lesion size • Malodor • Changes in skin color • Changes in skin temperature • Swelling in the foot or ankle • Open sores on the feet that are slow to heal or are draining • Ingrown toenails or toenails infected with fungus • Corns or calluses • Dry cracks in the skin, especially around the heel • Foot odor that is unusual or won't go away
- 10. NON- PHARMACOTHERAPY • Debridement of necrotic tissues • Wound drainage and amputation as required • Frequent dressing changes • Maximize glycemic control to aid in would healing • Elevation to decrease swelling
- 11. REAL CASE
- 12. SOAPANALYSIS • Patient Details- ➢Patient Name- ABC ➢IPN NO- IPD-1-220xxxx ➢Ward- General Surgery Male 410 ➢Date of Admission- 08-08-2022 ➢Date of Discharge- 20-08-2022 ➢Age- 47 years old ➢Gender- Male ➢Height- 170 CMS ➢Weight- 59 kg ➢BMI- 20.4 kg/m2 (Normal 18.5- 25)
- 13. SUBJECTIVE DATA • Chief Complaints- ➢Pain in the left great toe since 5-6 years and it is extending till ankle • Personal History- ➢Consumption of alcohol since 20 years, stopped consuming from last 3 years. ➢Chronic tobacco chewing since 25 years. • Medical History- Diabetes Mellitus type II • Medicine History- T. METFORMIN 2-0-1 • Diet-MIXED
- 14. OBJECTIVE DATA H/O- ➢Sudden onset non progressive ➢ Trauma ➢Purulent discharge ➢Fever and chills ➢Swelling in left Inguinal region ➢Local rise of temperature ➢Tenderness ➢Discoloration of toe since yesterday (i.e.- day before admission) O/E- ➢Conscious, Oriented, Afebrile
- 15. • Left lower limb DVT screening results- Subcutaneous edema is noted in left lower limb extending from mid leg to dorsum of foot. Lab reports- BLOOD GROUP O (RH POSITIVE) URINE ANALYSIS ABNORMAL VALUES NORMAL VALUES PROTIENS 2+ Absent SUGAR 2+ Absent PUS (WBC CELLS) 8-10 HPF Absent EPITHELIAL CELLS 7-8/HPF Absent
- 16. 25-OH VITAMIN D 15.10 Mild- moderate deficiency- 10-19ng/ml PROTHROMBIN TIME 15.30 10.56-13.37secs INR VALUE 1.27 0.85-1.15 SODIUM CHLORIDE 135 97 136-145mmol/Lt 98-107mmol/Lt ERYTHROCYTE SEDIMENTATION RATE 69 Upto 15mm/hr. BILIRUBIN TOTAL BILIRUBIN CONJUGATED 1.46 0.70 0.22-1.20mg/dl Upto 0.5 mg/dl WBC 18,900 4000-10000/uL MCHC 34.60 31.5- 34.5g/dl ABSOLUTE NEUTROPHILS 14,364 2000-7000/uL LYMPHOCYTES 13 20-40% ABSOLUTE MONOCYTES 1,890 200-1000/uL BLOOD SUGAR(RANDOM) 312 80-160 CRP 43.4mg/L 0-6.0
- 17. PRESCRIBED DRUGS DOSE ROUTE FREQUENCY DATE OF ADMINISTRATION INJ. TT 0.5ML IM STAT 8/8/22(1) INJ.TAXIM 1 GM IV 8 HOURLY 8/8/22(1) INJ. AUGMENTIN 1.2 GM IV 12 HOURLY 9/8/22-13/8/22 (2-6) INJ. PAN 40 MG IV 24 HOURLY 9/8/22-12/8/22 (2-5) INJ. DICLO 1 AMP IV 8 HOURLY 9/8/22-11/8/22(2-4) INJ. HAI 40IU SC 8 HOURLY 11/8/22-20/8/22(4-13) T. VITAMIN C 500MG ORAL 1-0-1 11/8/22- 20/8/22(4-13) C. MVBC 1 capsule ORAL 0-1-0 11/8/22- 20/8/22(4-13) T.PAN 40 MG ORAL 1-0-0 13/8/22- 20/8/22(6-13) T. EMAZEN D 50:10 MG ORAL 1-0-1 13/8/22- 20/8/22(6-13) Drug Chart- (DAYS)
- 18. PRESCRIBED DRUGS DOSE ROUTE FREQUENCY DATE OF ADMINISTRATION INJ. LANTUS 10U SC 1-0-0 13/8/22-20/8/22(6-13) INJ. PIPTAZ 4.5g IV 8 HOURLY 15/8/22-20/8/22(8-13) T. TELMA 40 MG ORAL 1-0-0 14/8/22- 20/8/22(7-13) Drug Chart-
- 19. ASSESSMENT • Diagnosis- Diabetic foot (left). • Etiology- 1. History of type II Diabetes Mellitus 2. Poor glycemic control 3. Improper foot care 4. Poor blood circulation 5. Dry skin 6. Impaired Immune response Due to excessive alcohol consumption and tobacco consumption which has lead to loss of essential nutrition from body.
- 20. • Progress chart- 8/8/022- L/E- local site of temp +, tenderness +, discharge+ O/E- conscious, oriented, afebrile Patient is comfortable PR- 84/min, BP- 140/80mmHg 9/8/22- L/E- local site of temp +, tenderness +, discharge+ O/E- conscious, oriented, afebrile Patient is comfortable PR- 87/min, BP- 160/80mmHg 10/8/022- L/E- no soakage O/C/O- amputation of left great toe SA. O/E- conscious, oriented, afebrile Patient is comfortable PR- 76/min, BP- 100/70mmHg 11/8/22- L/E- no soakage O/E- conscious, oriented, afebrile Patient is comfortable PR- 72/min, BP- 100/80mmHg
- 21. • Progress chart- 12/8/022- L/E- Healthy granulation tissue+ O/E- conscious, oriented, afebrile Patient is comfortable PR- 74/min, BP- 160/80mmHg 13/8/22- L/E- Healthy granulation tissue + O/E- conscious, oriented, afebrile Patient is comfortable PR- 74/min, BP- 160/90mmHg 14/8/022- L/E- Healthy granulation tissue with minimal slough+ O/E- conscious, oriented, afebrile Patient is comfortable PR- 82/min, BP- 140/90mmHg 15/8/22- L/E- Healthy granulation tissue with minimal slough+ O/E- conscious, oriented, afebrile Patient is comfortable PR- 78/min, BP- 130/80mmHg
- 22. • Progress chart- 16/8/022- L/E- Healthy granulation tissue + O/E- conscious, oriented, afebrile Patient is comfortable PR- 80/min, BP- 160/80mmHg 17/8/22- L/E- Healthy granulation tissue + O/E- conscious, oriented, afebrile Patient is comfortable PR- 76/min, BP- 150/80mmHg 18/8/022- L/E- Healthy granulation tissue + O/E- conscious, oriented, afebrile Patient is comfortable PR- 78/min, BP- 160/80mmHg 19/8/22- L/E- Wound Healthy O/E- conscious, oriented, afebrile Patient is comfortable PR- 76/min, BP- 160/80mmHg
- 23. • Progress chart- 20/8/22- L/E- Wound Healthy O/E- conscious, oriented, afebrile Patient is comfortable PR- 78/min, BP- 140/90mmHg • Operation Notes- Debridement SOS Amputation of left great toe SA. • Follow up details- ➢Visit daily for dressing, review back on Monday (22-8-22) in OPD 9 General Surgery or if needed SOS.
- 24. • Discharge medications- 1. C. MVBC 0-1-0 2. INJ.HAI 8-8-8U S/C 3. INJ. LANTUS 10U S/C @10PM 4. T.TELMA 40 MG 1-0-0 5. T.VITAMIN C 500MG 1-0-1 6. T.SHELCAL 500MG 0-1-0 FOR 15 DAYS 7. UPRISE D3 1 CAPSULE ONCE A WEEK FOR 4 WEEKS. 8. T. CEFIXIME 200MG 1-0-1 FOR 5 DAYS. 9. T. PAN 40 MG 1-0-0 FOR 5 DAYS.
- 25. • Goals achieved- 1. Symptomatic Improvement is seen. 2. Patient was hemodynamically stable at the time of discharge. 3. Operation conducted shown desired results. • Drugs to be avoided- When culture/ susceptibility test was done Proteus Vulagris bacteria found in discharge and it is resistant to drugs- AMPICILLIN, CEFAZOLIN, CEFUROXIME, TIGECYCLINE, TETRACYCLINE, NITROFURANTOIN, COLISTIN, POLYMYCIN B • Patient Compliance- ➢Patient didn’t have any complaints to the therapy given. • Response to therapy- ➢Patient responded well to therapy, symptoms were reduced.
- 26. INTERVENTION • Drug Interactions found between INJ. DICLO AND T. TELMA AII-RB may enhance toxic effect of NSAIDS, it can decrease GFR and renal function, severity is Moderate and there is to monitor that. • While prescribing drugs prescriber should mention drug generic name, instead of brand names.
- 27. MY PLAN- • Monitoring Parameters- 1. Blood sugar level 2. Symptoms like fever, itching on site 3. Local rise in temperature. • Drug Interactions- INJ. DICLO AND T. TELMA • Alternate therapy if any- CCBs- AMLODIPINE 10 MG ONCE DAILY- ORAL
- 28. PATIENT COUNSELLING- ➢On drugs- 1. T. VITAMIN C- Store in cool, dry, away from sunlight place. 2. C. MVBC- Don’t consume more than prescribed amount. 3. T.PAN 40- Consume 1 hr. before the meal.
- 29. ➢On disease- Follow Diabetic diet.
- 30. • Lifestyle Changes- 1. Stop alcohol and tobacco consumption. 2. Maintain regular schedule for eating and sleeping 3. Take medication on time, do not repeat dose if missed 4. Drink 7-8 glasses of water. 5. Avoid Junk food. 6. Consume protein rich foods- tofu, egg, chicken, seafood, lentils. 7. Consume whole grain and high fiber carbohydrates- beans, cereals, whole grain chapati 8. Consume non starchy vegetables- cauliflower, tomatoes, peppers, cabbage, French beans. 9. Consume 1:1 water and jamun and karela juice in the morning on an empty stomach.
- 31. BRAND NAMES PRESCRIBED DRUGS BRAND NAME 1. INJ. TT 2. INJ.TAXIM 3. INJ. AUGMENTIN 4. INJ. PAN 5. INJ. DICLO 6. INJ. HAI 7. T. VITAMIN C 8. C. MVBC 9. T. EMAZEN D 10. INJ. LANTUS 11. INJ. PIPTAZ 12. T. TELMA GENERIC NAME 1. TETANUS TOXOID 2. CEFOTAXIME 3. AMOXICILLIN/CLAVULANATE POTASSIUM 4. PANTOPRAZOLE 5. DICLOFENAAC 6. HUMAN ACTRAPID INSULIN 7. ASCORBIC ACID 8. MULTIVITAMIN 9. DICLOFENAC AND SERRATIOPEPTIDASE 10. INSULIN GLARGINE 11. PIPERACILLIN AND TAZOBACTAM 12. TELMISARTAN
- 32. REFERENCE 1. Diabetic foot treatment: Here's all you need to know about stem cell therapy. Hindustan Times. 2022 2. Pendsey SP. Understanding diabetic foot. International journal of diabetes in developing countries. Medknow Publications; 2010. 3. Justin J. Sherman MCS. Diabetic foot ulcer assessment and treatment: A pharmacist's guide. U.S. Pharmacist– The Leading Journal in Pharmacy. 2010. 4. Diabetic foot problems: Symptoms, treatment, and care. WebMD. 5. Oluwaranti Akiyode PD. Management of acute diabetic foot disease. U.S. Pharmacist–The Leading Journal in Pharmacy.2014 6. Aims & primary goals. Diabetic Foot Clinic. 2020 7. Online. Lexicomp Online. 8. Hmpgloballearningnetwork.com. 9. Explore scientific, technical, and medical research on ScienceDirect. ScienceDirect.com | Science, health and medical journals, full text articles and books.