Downloaded 374 times
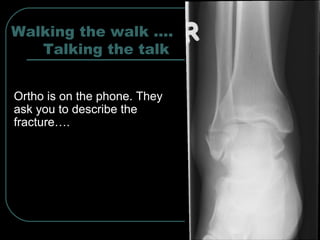
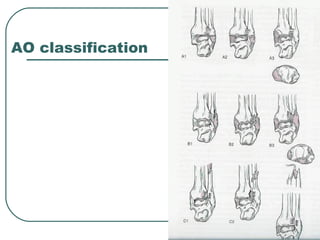


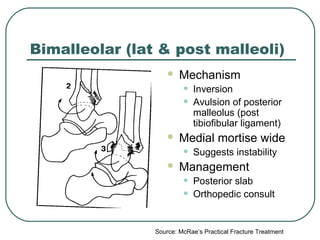



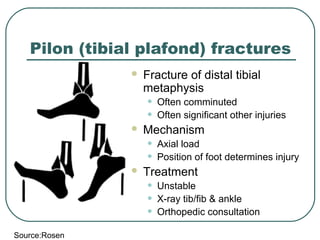


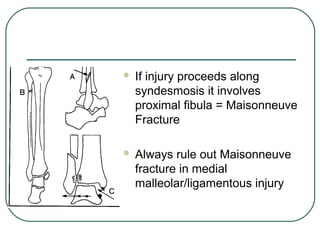
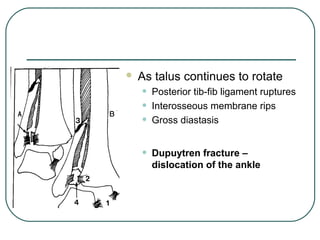


The document discusses common ankle fractures, including: - Lateral malleolar fractures (Danis-Weber type A), which are stable and treated with casting. - Bimalleolar fractures involving the lateral and posterior malleoli, which can be unstable and require orthopedic consultation. - Trimalleolar fractures, which are highly unstable with multiple ligament injuries and usually involve the syndesmosis, requiring orthopedic surgery. - Pilon fractures of the distal tibia are often comminuted with significant injuries requiring orthopedic consultation. - Tillaux fractures in adolescents involve the anterolateral physis and epiphysis and require orthopedic consultation to ensure proper















































