List of contents
•Introduction
• Peculiarities of TM Joint.
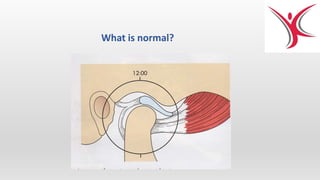
• Applied anatomy.
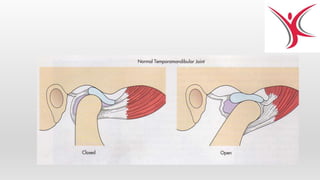
• Normal movements.
• Evaluation of patient.
• Signs and symptoms
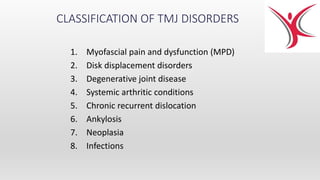
• Classification of TMJ disorders.
• A brief insight into
MPDS.
Internal derangements.
Dislocations, subluxation.
Ankylosis.
Introduction
All the bonesin the skull are attached with fibrous joint
and are immovable expect for temporomandibular joint.
• The temporomandibular joint( TMJ ) is a bilateral synovial
articulation between the mandible and temporal bone. The
name of the joint is derived from the two bones which
form the joint: the upper temporal bone which is part of
the cranium (skull), and the lower jawbone or mandible.
• The most important functions of the
temporomandibular joint (TMJ) are mastication and
speech.
1/7/2018 SEMINAR ON APPLIED ANATOMY OF TMJ, G.Guru Karthik/91 5
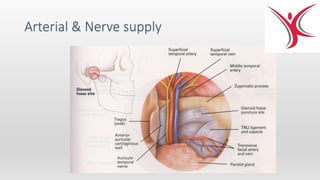
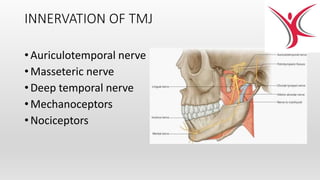
INNERVATION OF TMJ
•Auriculotemporal nerve
• Masseteric nerve
• Deep temporal nerve
• Mechanoceptors
• Nociceptors
12.
Peculiarities of TMJ
1.Bilateral diarthrosis – right & left function together
2. Articular surface covered by fibrocartilage instead of
hyaline cartilage.
3. Only joint in human body to have a rigid endpoint of
closure i.e. occlusal contact through teeth.
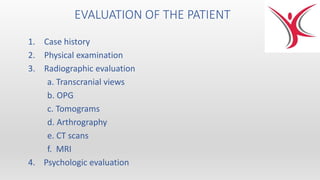
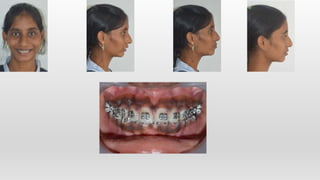
EVALUATION OF THEPATIENT
1. Case history
2. Physical examination
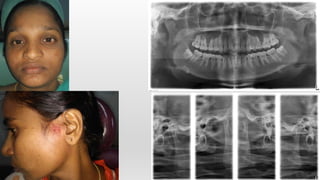
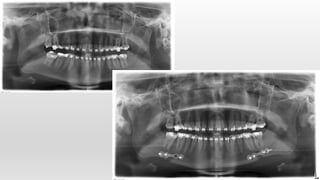
3. Radiographic evaluation
a. Transcranial views
b. OPG
c. Tomograms
d. Arthrography
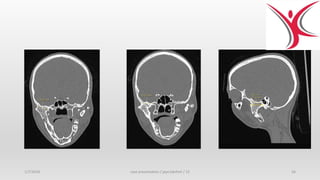
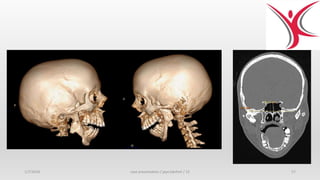
e. CT scans
f. MRI
4. Psychologic evaluation
17.
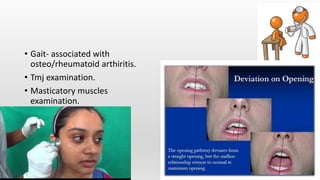
1. History oftrauma.
2. History of rheumatoid arthiritis.
3. History of osteoarthritis.
4. History of long standing otitis
media.
5. Long standing cervical spondylitis.
6. History of extraction of posterior
teeth.
7. Bruxism.
8. History of psychological issues.
9. History of unfinished orthodontic
treatment.
MYOFASCIAL PAIN &DYSFUNCTON
•MPD is the most common cause of
masticatory pain and limited function for
which patients seek dental consultation
and treatment.
•The source of the pain and dysfunction is
muscular, with masticatory muscles
developing tenderness and pain as a
result of abnormal muscular function or
hyperactivity.
MYOFASCIAL PAIN &DYSFUNCTON
SIGNS :
• Diffuse tenderness of the masticatory muscles
• The range of the mandibular movements is
decreased
• Deviation of the mandible to the affected side
• The teeth frequently have wear facets
• Joint noises may be present
• Trismus.
• Radiographs of the TMJs are usually normal
27.
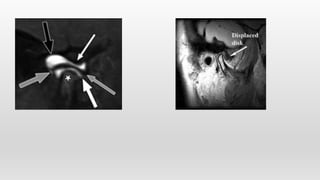
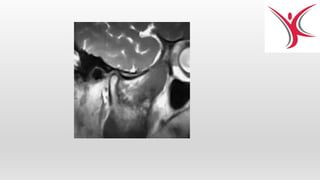
2. DISC DISPLACEMENTDISORDERS
Disk displacement with reduction Disk displacement without reduction
ARTHROCENTESIS
• L.A. withintravenous sedation
• Needles into the superior joint space
• Ringer’s solution
• Steroids, L.A
• NSAIDs
• Very effective in anterior disk displacement without
reduction
• Stretching of capsule, decrease in pain mediators,
release of adhesions, elimination of negative
pressure
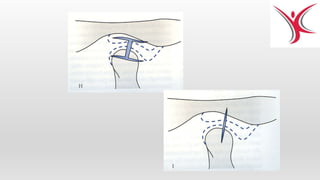
DISK REPOSITIONING SURGERY
•Indicated in anterior disk displacement with or
without reduction
• Removing a wedge of tissue from posterior
attachment
• Suturing the disk back to the correct anatomical
position
• May be combined with recontouring of the
disk,articular eminence,and condyle
• Jaw exercises
39.
DISK REPAIR ORREMOVAL
• Disk repair with dermal grafts or fascial tissue
• Diskectomy without replacement
• Disk replacement with autogenous grafts or
alloplastic implants
40.
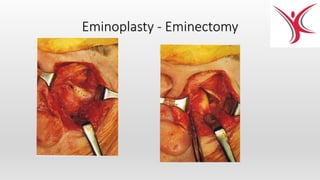
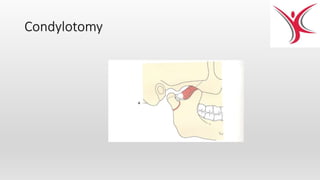
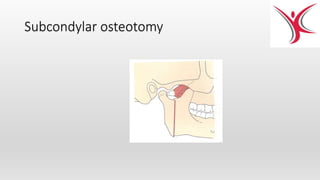
MANAGEMENT OF RECURRENT
DISLOCATION
1.Capsule tightening procedures
(capsulorrhaphy,reinforcement of capsule)
2. Creating mechanical obstacle
(osteotomy of eminence,placement of
graft,silastic block,Dautry’s procedure,
use of pins or screws)
3. Direct restrain of condyle
4. Creation of new muscle balance
5. Removal of mechanical obstacles
OUR TEAM
Dr. SrinivasSakamuri MDS Endodontist
Dr Sahana Mallineni MDS Periodeontist
Dr. Venkatesh Nettam MDS Orthodontist
Dr. Kalyani Ch. BDS EHS Coordinator
Dr. Chandana BDS Budding Dentist
Dr. G. Guru Karthik MDS Oral and Maxillofacial Surgeon