Downloaded 65 times





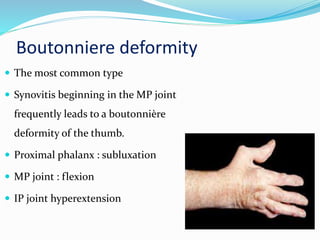




















Rheumatoid arthritis is a common inflammatory joint disease that can lead to joint deformities. The document discusses common thumb deformities caused by RA like boutonniere and swan neck deformities. Treatment options range from splinting and synovectomy for mild cases to joint fusion or arthroplasty for more severe deformities. Tendon ruptures are also addressed along with surgical techniques like tendon transfers to restore function.



































































