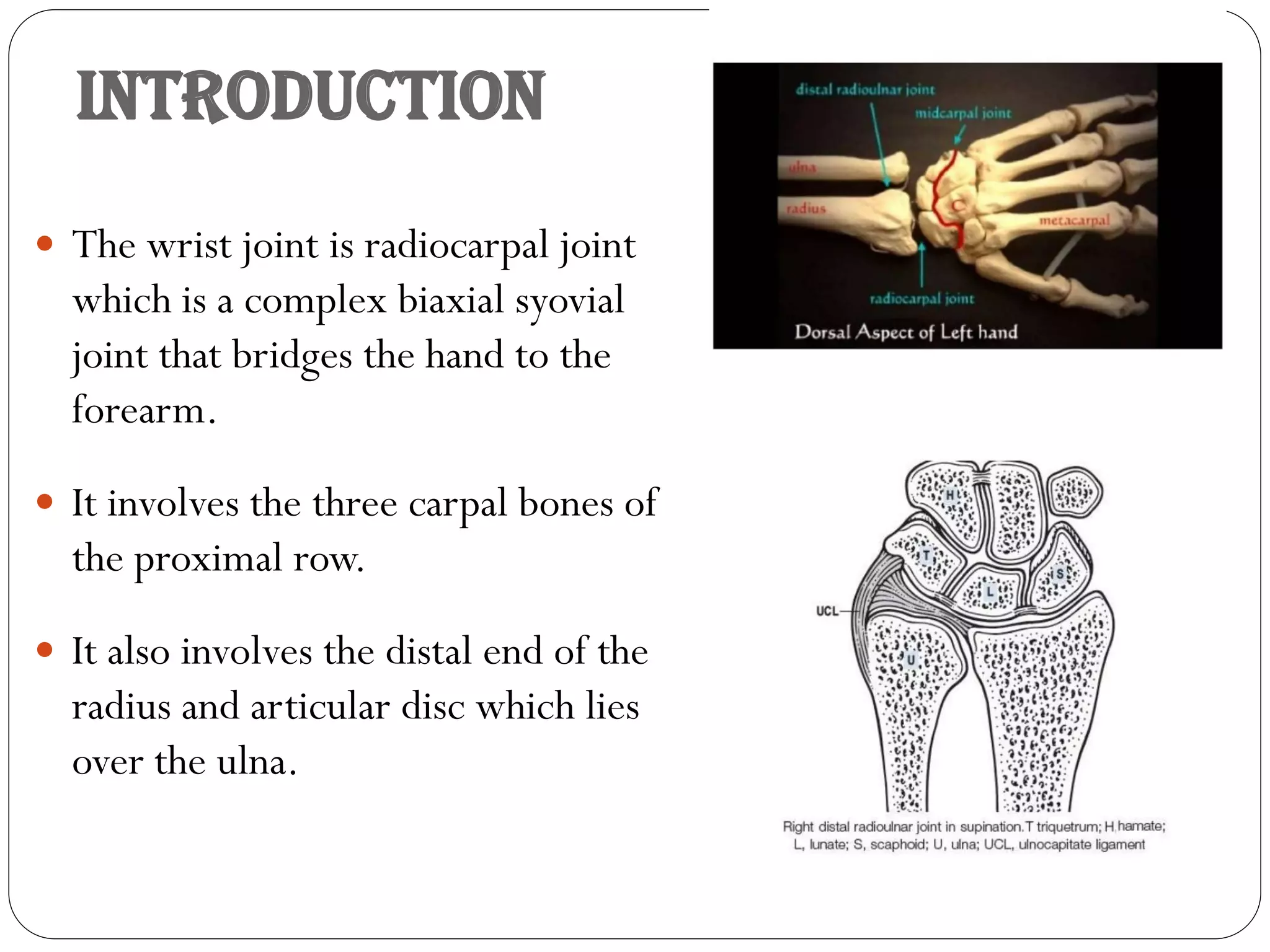
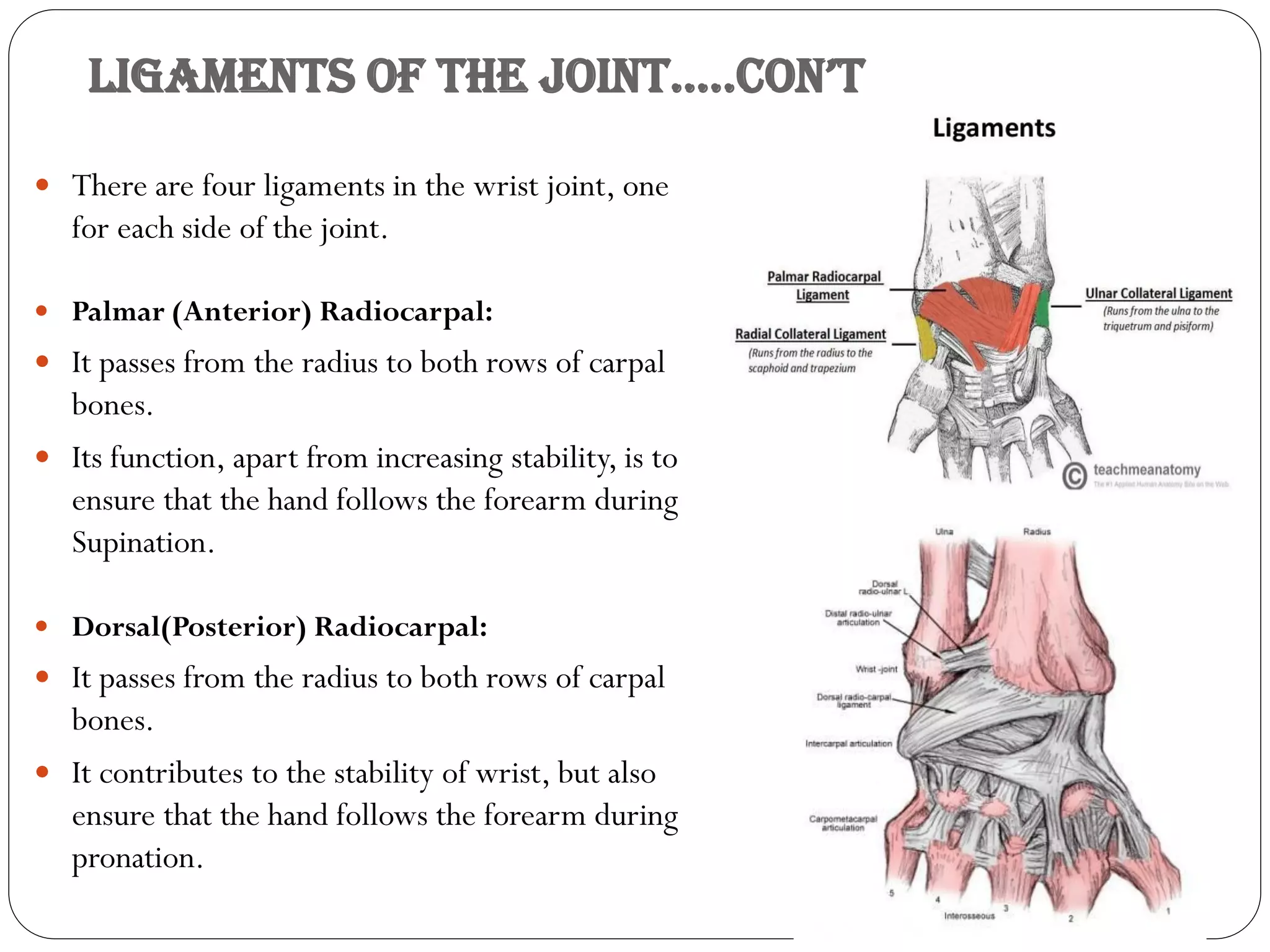
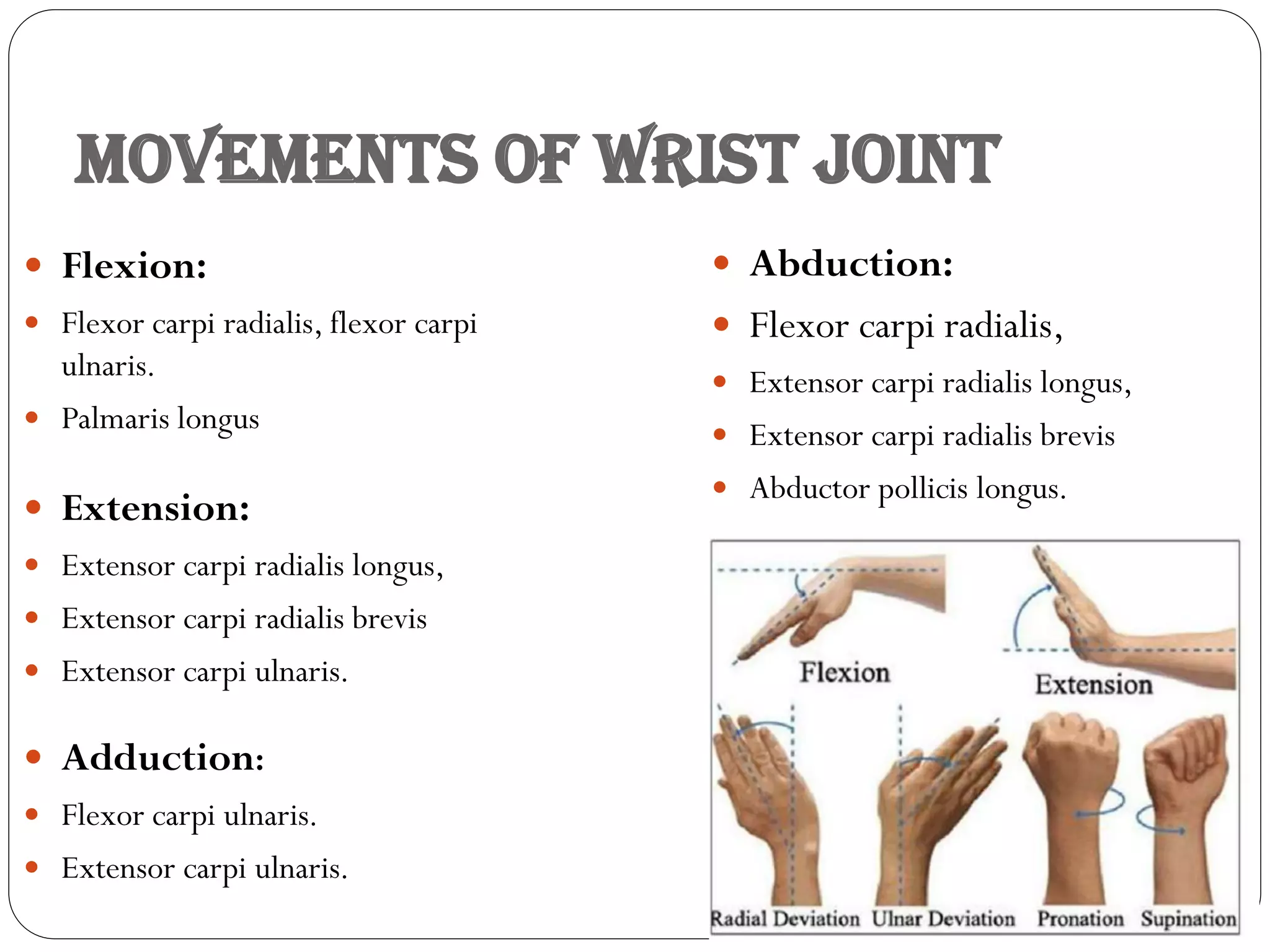
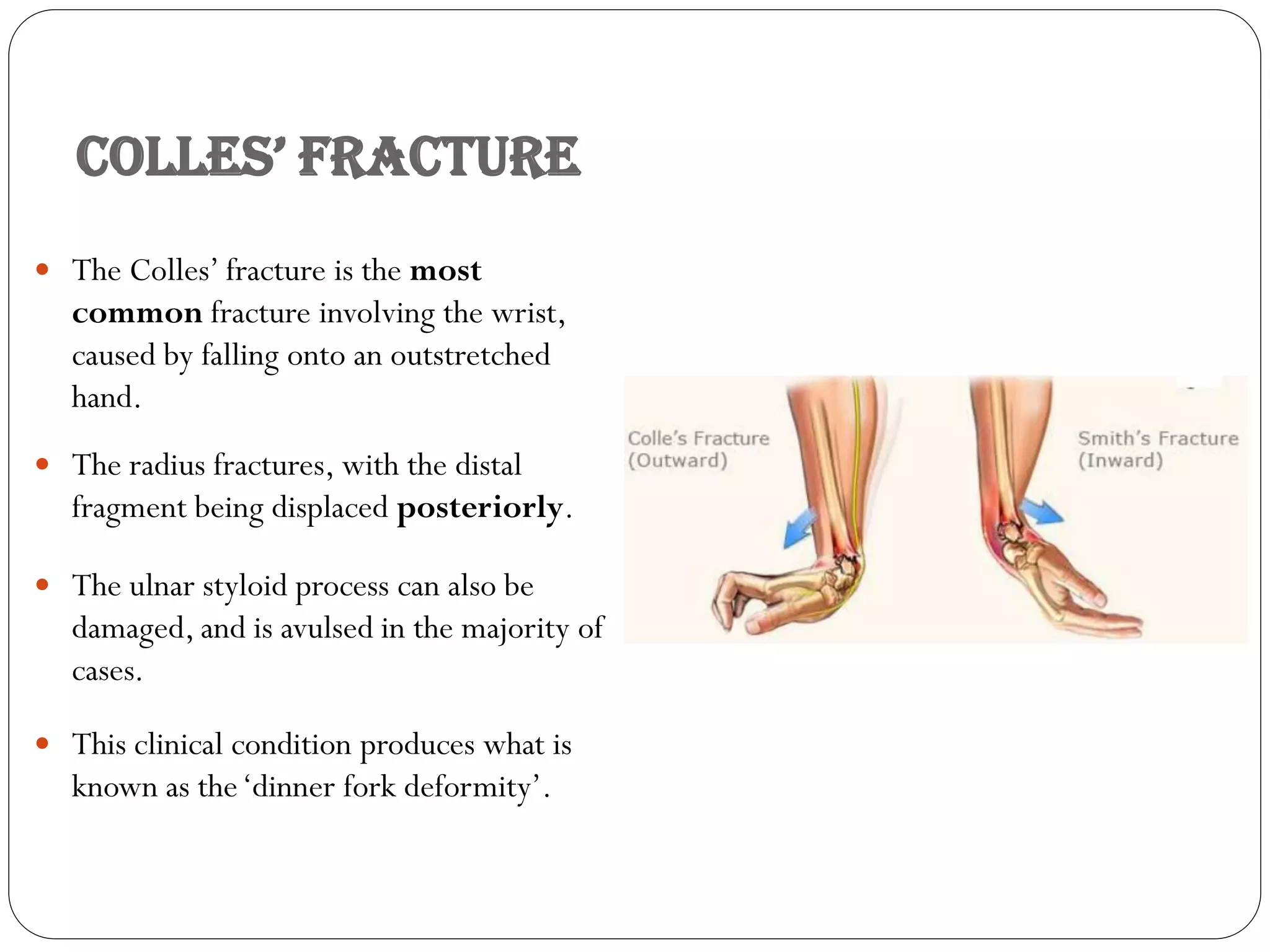
The wrist joint is a complex biaxial joint between the carpal bones and the distal end of the radius. It allows for flexion/extension and abduction/adduction motions. Key structures include the articular surfaces of the radius, triangular articular disc, and proximal carpal bones. The joint is surrounded by ligaments including the radial and ulnar collateral ligaments. Common injuries include fractures of the scaphoid bone and Colles' fracture of the radius. Ganglions also sometimes develop as cysts near the joint.