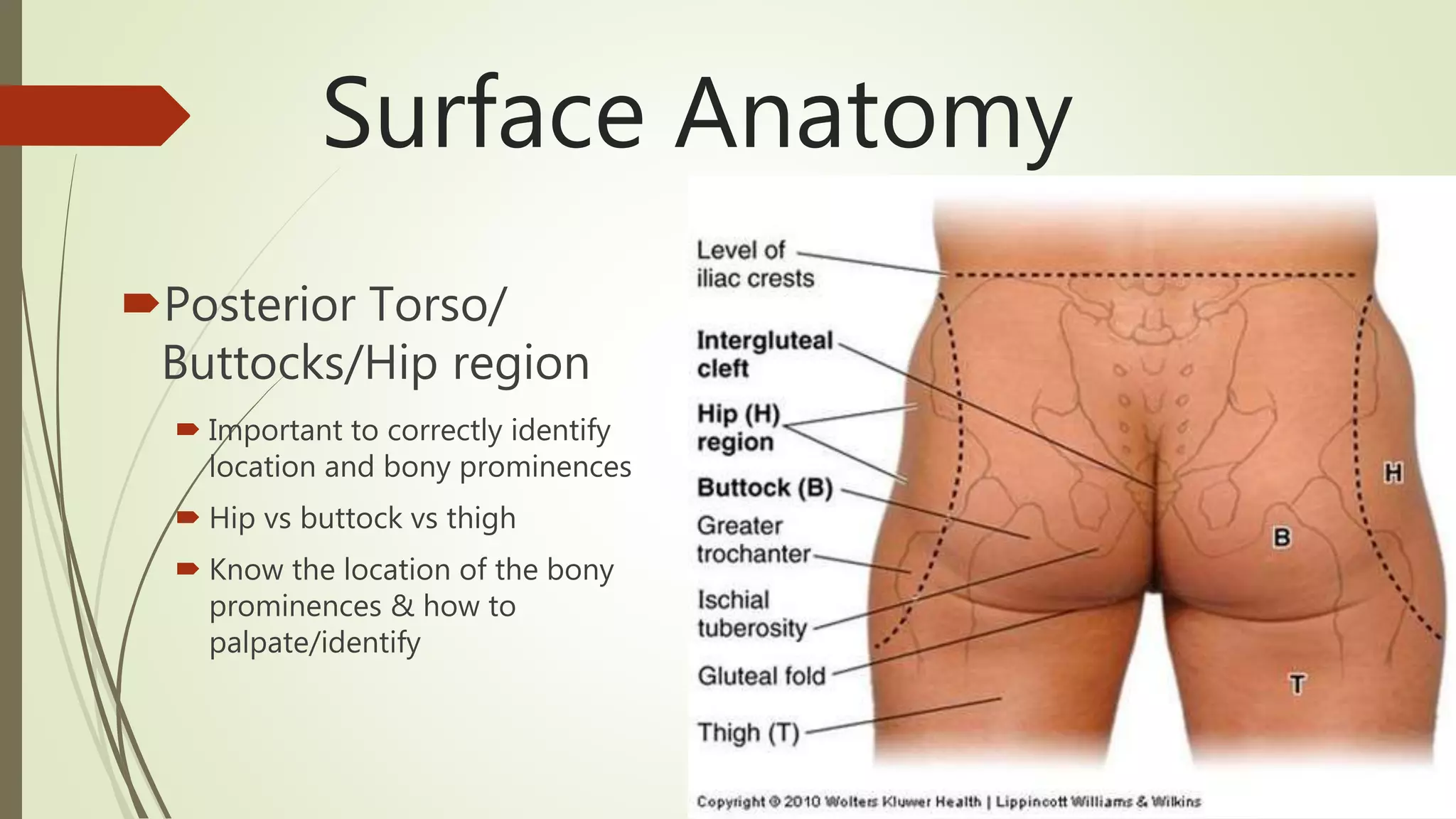
Wound documentation is important for clarity and to avoid misunderstanding. Location should use correct anatomical terminology like dorsal vs. plantar on the foot. Size is measured in centimeters with length, width, and depth. Photography can support written documentation if institutional policy is followed, using a measuring device and macro mode for close-up shots without distortion.