Downloaded 210 times



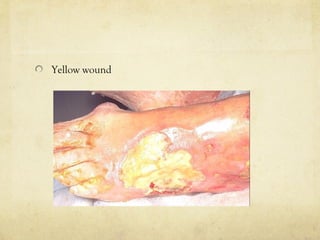
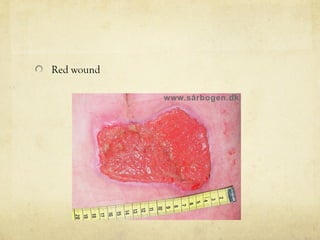
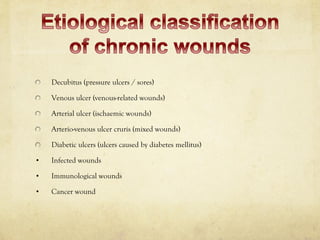
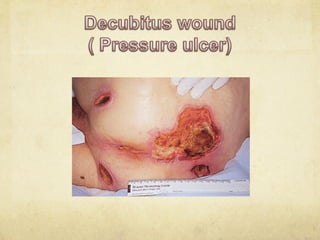
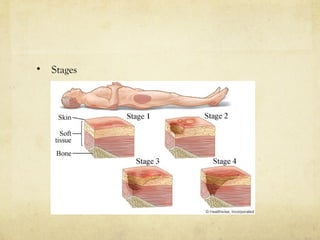
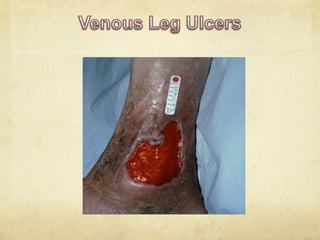




The document discusses the history of wound care from ancient times to modern practices. Some key points covered include: - Ancient civilizations used remedies like honey, grease, and herbs to treat wounds. Hippocrates advocated cleaning wounds with wine or vinegar. - Different types of wounds are discussed like acute, chronic, pressure ulcers, venous ulcers, and diabetic foot ulcers. - Modern wound care includes debridement, dressings, antibiotics, growth factors, skin substitutes, and addressing underlying patient issues. - Wound etiology, staging, and treatments are described for various chronic wounds. Biofilms, infection, and other complex wound factors are also addressed.



































































![Skin integrity and wound care [autosaved] (2)](https://cdn.slidesharecdn.com/ss_thumbnails/skinintegrityandwoundcareautosaved2-130319145819-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)

























