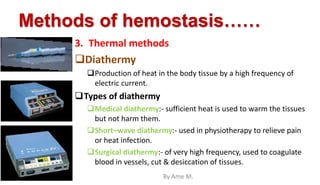
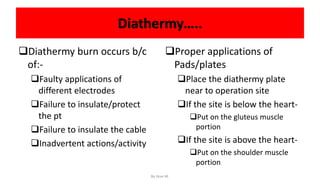
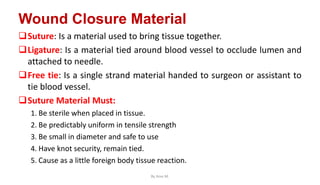
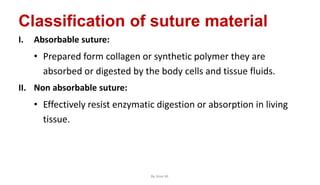
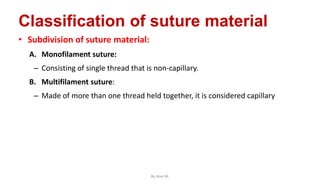
This document discusses wound care and healing over multiple pages. It covers the wound healing process, different types of wounds and wound healing, methods of hemostasis including chemical, mechanical, and thermal methods like diathermy. It also discusses factors that influence wound healing and choices of suture materials based on wound and patient characteristics. Proper hand hygiene for wound care is also emphasized.





















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)