Download as PDF, PPTX




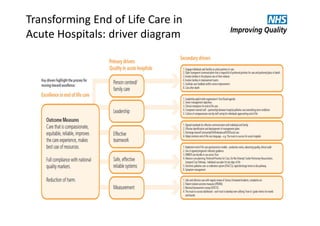
![82,060,422 outpatient appointments
in 1 year in England [5]
10% of these were attended by patients aged 80+
36% of the Welsh population had an
outpatient appointment [6]
Emergency readmissions within 30 days are
high xx for patients who had a period of uncertainty during their
inpatient stay who died within 100 days of discharge.
33% of around 10,000
incidents related to
discharge in 2012/13 were
due to communication at
handover. England [9]
One third of patients die during the one year
follow‐up period. 9.3% of all patients died in
the admission period. 25 Scottish Teaching Hospitals [2]
Systematic review showed variation in
home preference estimates ranged
31% to 87% for patients (9 studies),
25% to 64% for caregivers (5 studies),
49% to 70% for the public (4 studies).
[3]
Studies included in our efficacy
analysis of advance care planning
were all conducted in an outpatient
setting during scheduled visits. [4]
How well pain was relieved during the last three months of life, England, 2013 [7]
Around half of the 570,000 people who
die in the UK each year, die in hospital [1]
25% patients who receive ICU / HDU
care are near end of their lives . Around 30k
patients admitted to ICU/HDU in Scotland. Around
16% receive last days of life care in the unit. A further
9% die in a general ward/ post discharge. [8]
On average there were xx
emergency readmissions per
acute hospital in 2011.](https://image.slidesharecdn.com/workshop6-workingtogether-buildingonthebest-151221165957/85/Transforming-End-of-Life-Care-in-Acute-Hospitals-PM-Workshop-6-Working-together-Building-on-the-best-9-320.jpg)
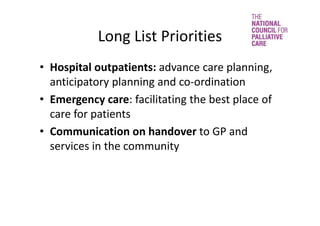
!["Those with experience
of relatives dying in
hospitals report
the medical support is
not as good as expected,
while personal support is
poor, but as expected."
Sue Ryder, a time and a
place[12]
69% of bereaved people whose relative or friend died in a
hospital, rated care as outstanding, excellent or good. Significantly
lower than hospice (83%), care home (82%) or at home (79%). England,
VOICES‐SF survey
33% reported that the hospital services did not
work well together with GP and other services outside the
hospital. England VOICES‐SF survey [7]
some aspects of the dying
environment as being more
important than physical
location. [11] Choice
report
More than 73% respondents felt
hospital was the right place for their
friend or relative to die, despite only 3%
of all respondents stating patients
wanted to die in hospital. [7]
“Sometimes, it's
the little things
that matter, and
that is what you
remember.”
Expert with lived experience. [10]
While the majority said choice is important, many
said an important consideration was quality. [11]
Themes from ombudsman report [13]
•Not recognising people are dying, not responding to
need
•Poor symptom control
•Poor communication
•Poor care planning (hospitals and GPs liaise)
•Delays in diagnosis
Hospital staff received
the lowest
proportion always
showing dignity and
respect (58% for
hospital doctors and 51%
for hospital nurses). [7]
Most bereaved people did not
talk to anyone from any support
services since the death, most.
18% said they had not, but
would have liked to. VOICES‐SF](https://image.slidesharecdn.com/workshop6-workingtogether-buildingonthebest-151221165957/85/Transforming-End-of-Life-Care-in-Acute-Hospitals-PM-Workshop-6-Working-together-Building-on-the-best-10-320.jpg)

The document outlines initiatives to enhance end-of-life care in acute hospitals, focusing on areas such as advance care planning, partnerships, and resource utilization. It highlights the National Council for Palliative Care's role in influencing government policy and improving public awareness about dying and bereavement. Key priorities include better communication among healthcare providers, improved pain management, and ensuring patients receive care in their preferred environments.










































































































