Periprosthetic fractures are the third most common reason for revision total hip arthroplasty. Surgical treatment of periprosthetic fractures belongs to the most difficult procedures due to the extensive surgery, elderly polymorbid patients and the high frequency of other complications. The aim of this study was to evaluate the results of operatively treated periprosthetic femoral fractures after total hip arthroplasty.
We evaluated 47 periprosthetic fractures in 40 patients (18 men and 22 women) operated on between January 2004 and December 2010. The mean follow-up period was 27 months (within a range of 12-45 months). For the clinical evaluation, we used modified Merle d'Aubigné scoring system.
In group of Vancouver A fractures, 3 patients were treated with a mean score of 15,7 points (good result). We recorded a mean score of 14,2 points (fair result) in 6 patients with Vancouver B1 fractures, 12,4 points (fair result) in 24 patients with Vancouver B2 fractures and 12,8 points (fair result) in 7 patients with Vancouver B3 fractures. In group of Vancouver C fractures, we found a mean score of 16,2 points (good result) in 7 patients.
Therapeutic algorithm based on the Vancouver classification system is, in our opinion, satisfactory. Accurate differentiation of B1 and B2 type of fractures is essential. Preoperative radiographic images may not be reliable and checking the stability of the prosthesis fixation during surgery should be performed.
Corrective Surgery for Malunited Tibial Plateau Fractureiosrjce
IOSR Journal of Dental and Medical Sciences is one of the speciality Journal in Dental Science and Medical Science published by International Organization of Scientific Research (IOSR). The Journal publishes papers of the highest scientific merit and widest possible scope work in all areas related to medical and dental science. The Journal welcome review articles, leading medical and clinical research articles, technical notes, case reports and others.
Periprosthetic fractures are the third most common reason for revision total hip arthroplasty. Surgical treatment of periprosthetic fractures belongs to the most difficult procedures due to the extensive surgery, elderly polymorbid patients and the high frequency of other complications. The aim of this study was to evaluate the results of operatively treated periprosthetic femoral fractures after total hip arthroplasty.
We evaluated 47 periprosthetic fractures in 40 patients (18 men and 22 women) operated on between January 2004 and December 2010. The mean follow-up period was 27 months (within a range of 12-45 months). For the clinical evaluation, we used modified Merle d'Aubigné scoring system.
In group of Vancouver A fractures, 3 patients were treated with a mean score of 15,7 points (good result). We recorded a mean score of 14,2 points (fair result) in 6 patients with Vancouver B1 fractures, 12,4 points (fair result) in 24 patients with Vancouver B2 fractures and 12,8 points (fair result) in 7 patients with Vancouver B3 fractures. In group of Vancouver C fractures, we found a mean score of 16,2 points (good result) in 7 patients.
Therapeutic algorithm based on the Vancouver classification system is, in our opinion, satisfactory. Accurate differentiation of B1 and B2 type of fractures is essential. Preoperative radiographic images may not be reliable and checking the stability of the prosthesis fixation during surgery should be performed.
Corrective Surgery for Malunited Tibial Plateau Fractureiosrjce
IOSR Journal of Dental and Medical Sciences is one of the speciality Journal in Dental Science and Medical Science published by International Organization of Scientific Research (IOSR). The Journal publishes papers of the highest scientific merit and widest possible scope work in all areas related to medical and dental science. The Journal welcome review articles, leading medical and clinical research articles, technical notes, case reports and others.
Dr. Ahmed M. Adawy, Professor Emeritus, Dep. Oral & Maxillofacial Surgery. Former Dean, Faculty of Dental Medicine, Al-Azhar University. Mandibular angle fractures account for 23% to 42% of all facial fractures. Fracture of mandibular angle can be classified as (A) Vertical favorable or unfavorable, (B) Horizontally favorable of unfavorable. Traditionally, mandibular angle fractures have been treated with either closed reduction and inter-maxillary fixation or open reduction and internal fixation with or without inter-maxillary fixation. Patients treated with inter-maxillary fixation have a restricted airway and loose excess weight. Rigid internal fixation and early return to function have eliminated the use of wire osteosenthysis and prolonged use of inter-maxillary fixation. The principal of rigid fixation, however, have inherent set of disadvantages including damage to the inferior alveolar nerve and the marginal mandibular branch of facial nerve. Postoperative malocclusion rates are also high. With the introduction of semi-rigid technique fracture of the mandibular angle could be treated according to Champy’s Ideal lines of osteosenthysis. The technique involves placement of a single monocortial miniplate on the superior border of the mandible. However, some studies suggested using a second miniplate along the inferior border. Wether one or two miniplates should be used is still debatable. The application of 3D plates may provide additional stability in 3 dimension and good resistance against torque forces.
MIROS (Minimally Invasive Reduction and Osteosynthesis System®)CHAUDHARY ARPAN
MIROS (Minimally Invasive Reduction and Osteosynthesis System
MIROS consists of four 2.5 mm thick and 50 cm long stainless steel or titanium wires the end
of which is introduced into a metallic clip.
Assumed that the MIROS might provide greater fracture stability and less complications
with respect to traditional percutaneous pinning (TPP).
Slides from Prof Dan Pratt presented at the Teaching to Teach Workshop in Boston, MA, May 1-2, 2009;
Massachusetts General Hospital, Harvard Medical School.
Report Back from SGO 2024: What’s the Latest in Cervical Cancer?bkling
Are you curious about what’s new in cervical cancer research or unsure what the findings mean? Join Dr. Emily Ko, a gynecologic oncologist at Penn Medicine, to learn about the latest updates from the Society of Gynecologic Oncology (SGO) 2024 Annual Meeting on Women’s Cancer. Dr. Ko will discuss what the research presented at the conference means for you and answer your questions about the new developments.
Flu Vaccine Alert in Bangalore Karnatakaaddon Scans
As flu season approaches, health officials in Bangalore, Karnataka, are urging residents to get their flu vaccinations. The seasonal flu, while common, can lead to severe health complications, particularly for vulnerable populations such as young children, the elderly, and those with underlying health conditions.
Dr. Vidisha Kumari, a leading epidemiologist in Bangalore, emphasizes the importance of getting vaccinated. "The flu vaccine is our best defense against the influenza virus. It not only protects individuals but also helps prevent the spread of the virus in our communities," he says.
This year, the flu season is expected to coincide with a potential increase in other respiratory illnesses. The Karnataka Health Department has launched an awareness campaign highlighting the significance of flu vaccinations. They have set up multiple vaccination centers across Bangalore, making it convenient for residents to receive their shots.
To encourage widespread vaccination, the government is also collaborating with local schools, workplaces, and community centers to facilitate vaccination drives. Special attention is being given to ensuring that the vaccine is accessible to all, including marginalized communities who may have limited access to healthcare.
Residents are reminded that the flu vaccine is safe and effective. Common side effects are mild and may include soreness at the injection site, mild fever, or muscle aches. These side effects are generally short-lived and far less severe than the flu itself.
Healthcare providers are also stressing the importance of continuing COVID-19 precautions. Wearing masks, practicing good hand hygiene, and maintaining social distancing are still crucial, especially in crowded places.
Protect yourself and your loved ones by getting vaccinated. Together, we can help keep Bangalore healthy and safe this flu season. For more information on vaccination centers and schedules, residents can visit the Karnataka Health Department’s official website or follow their social media pages.
Stay informed, stay safe, and get your flu shot today!
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Ve...kevinkariuki227
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
Factory Supply Best Quality Pmk Oil CAS 28578–16–7 PMK Powder in Stockrebeccabio
Factory Supply Best Quality Pmk Oil CAS 28578–16–7 PMK Powder in Stock
Telegram: bmksupplier
signal: +85264872720
threema: TUD4A6YC
You can contact me on Telegram or Threema
Communicate promptly and reply
Free of customs clearance, Double Clearance 100% pass delivery to USA, Canada, Spain, Germany, Netherland, Poland, Italy, Sweden, UK, Czech Republic, Australia, Mexico, Russia, Ukraine, Kazakhstan.Door to door service
Hot Selling Organic intermediates
Couples presenting to the infertility clinic- Do they really have infertility...Sujoy Dasgupta
Dr Sujoy Dasgupta presented the study on "Couples presenting to the infertility clinic- Do they really have infertility? – The unexplored stories of non-consummation" in the 13th Congress of the Asia Pacific Initiative on Reproduction (ASPIRE 2024) at Manila on 24 May, 2024.
Ethanol (CH3CH2OH), or beverage alcohol, is a two-carbon alcohol
that is rapidly distributed in the body and brain. Ethanol alters many
neurochemical systems and has rewarding and addictive properties. It
is the oldest recreational drug and likely contributes to more morbidity,
mortality, and public health costs than all illicit drugs combined. The
5th edition of the Diagnostic and Statistical Manual of Mental Disorders
(DSM-5) integrates alcohol abuse and alcohol dependence into a single
disorder called alcohol use disorder (AUD), with mild, moderate,
and severe subclassifications (American Psychiatric Association, 2013).
In the DSM-5, all types of substance abuse and dependence have been
combined into a single substance use disorder (SUD) on a continuum
from mild to severe. A diagnosis of AUD requires that at least two of
the 11 DSM-5 behaviors be present within a 12-month period (mild
AUD: 2–3 criteria; moderate AUD: 4–5 criteria; severe AUD: 6–11 criteria).
The four main behavioral effects of AUD are impaired control over
drinking, negative social consequences, risky use, and altered physiological
effects (tolerance, withdrawal). This chapter presents an overview
of the prevalence and harmful consequences of AUD in the U.S.,
the systemic nature of the disease, neurocircuitry and stages of AUD,
comorbidities, fetal alcohol spectrum disorders, genetic risk factors, and
pharmacotherapies for AUD.
MANAGEMENT OF ATRIOVENTRICULAR CONDUCTION BLOCK.pdfJim Jacob Roy
Cardiac conduction defects can occur due to various causes.
Atrioventricular conduction blocks ( AV blocks ) are classified into 3 types.
This document describes the acute management of AV block.
micro teaching on communication m.sc nursing.pdfAnurag Sharma
Microteaching is a unique model of practice teaching. It is a viable instrument for the. desired change in the teaching behavior or the behavior potential which, in specified types of real. classroom situations, tends to facilitate the achievement of specified types of objectives.
HOT NEW PRODUCT! BIG SALES FAST SHIPPING NOW FROM CHINA!! EU KU DB BK substit...GL Anaacs
Contact us if you are interested:
Email / Skype : kefaya1771@gmail.com
Threema: PXHY5PDH
New BATCH Ku !!! MUCH IN DEMAND FAST SALE EVERY BATCH HAPPY GOOD EFFECT BIG BATCH !
Contact me on Threema or skype to start big business!!
Hot-sale products:
NEW HOT EUTYLONE WHITE CRYSTAL!!
5cl-adba precursor (semi finished )
5cl-adba raw materials
ADBB precursor (semi finished )
ADBB raw materials
APVP powder
5fadb/4f-adb
Jwh018 / Jwh210
Eutylone crystal
Protonitazene (hydrochloride) CAS: 119276-01-6
Flubrotizolam CAS: 57801-95-3
Metonitazene CAS: 14680-51-4
Payment terms: Western Union,MoneyGram,Bitcoin or USDT.
Deliver Time: Usually 7-15days
Shipping method: FedEx, TNT, DHL,UPS etc.Our deliveries are 100% safe, fast, reliable and discreet.
Samples will be sent for your evaluation!If you are interested in, please contact me, let's talk details.
We specializes in exporting high quality Research chemical, medical intermediate, Pharmaceutical chemicals and so on. Products are exported to USA, Canada, France, Korea, Japan,Russia, Southeast Asia and other countries.
These simplified slides by Dr. Sidra Arshad present an overview of the non-respiratory functions of the respiratory tract.
Learning objectives:
1. Enlist the non-respiratory functions of the respiratory tract
2. Briefly explain how these functions are carried out
3. Discuss the significance of dead space
4. Differentiate between minute ventilation and alveolar ventilation
5. Describe the cough and sneeze reflexes
Study Resources:
1. Chapter 39, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 34, Ganong’s Review of Medical Physiology, 26th edition
3. Chapter 17, Human Physiology by Lauralee Sherwood, 9th edition
4. Non-respiratory functions of the lungs https://academic.oup.com/bjaed/article/13/3/98/278874
Explore natural remedies for syphilis treatment in Singapore. Discover alternative therapies, herbal remedies, and lifestyle changes that may complement conventional treatments. Learn about holistic approaches to managing syphilis symptoms and supporting overall health.
New Directions in Targeted Therapeutic Approaches for Older Adults With Mantl...i3 Health
i3 Health is pleased to make the speaker slides from this activity available for use as a non-accredited self-study or teaching resource.
This slide deck presented by Dr. Kami Maddocks, Professor-Clinical in the Division of Hematology and
Associate Division Director for Ambulatory Operations
The Ohio State University Comprehensive Cancer Center, will provide insight into new directions in targeted therapeutic approaches for older adults with mantle cell lymphoma.
STATEMENT OF NEED
Mantle cell lymphoma (MCL) is a rare, aggressive B-cell non-Hodgkin lymphoma (NHL) accounting for 5% to 7% of all lymphomas. Its prognosis ranges from indolent disease that does not require treatment for years to very aggressive disease, which is associated with poor survival (Silkenstedt et al, 2021). Typically, MCL is diagnosed at advanced stage and in older patients who cannot tolerate intensive therapy (NCCN, 2022). Although recent advances have slightly increased remission rates, recurrence and relapse remain very common, leading to a median overall survival between 3 and 6 years (LLS, 2021). Though there are several effective options, progress is still needed towards establishing an accepted frontline approach for MCL (Castellino et al, 2022). Treatment selection and management of MCL are complicated by the heterogeneity of prognosis, advanced age and comorbidities of patients, and lack of an established standard approach for treatment, making it vital that clinicians be familiar with the latest research and advances in this area. In this activity chaired by Michael Wang, MD, Professor in the Department of Lymphoma & Myeloma at MD Anderson Cancer Center, expert faculty will discuss prognostic factors informing treatment, the promising results of recent trials in new therapeutic approaches, and the implications of treatment resistance in therapeutic selection for MCL.
Target Audience
Hematology/oncology fellows, attending faculty, and other health care professionals involved in the treatment of patients with mantle cell lymphoma (MCL).
Learning Objectives
1.) Identify clinical and biological prognostic factors that can guide treatment decision making for older adults with MCL
2.) Evaluate emerging data on targeted therapeutic approaches for treatment-naive and relapsed/refractory MCL and their applicability to older adults
3.) Assess mechanisms of resistance to targeted therapies for MCL and their implications for treatment selection
New Directions in Targeted Therapeutic Approaches for Older Adults With Mantl...
Wiring Tibial Tubercle Fractures
1. P A R T N E R S O R T H O P A E D I C
Trauma Rounds
Case Reports from the Mass General Hospital and Brigham &Women’s Hospital
A Quarterly Case Study Volume 1, Fall 2009
Wiring Tibial Tubercle Fractures
Mark Vrahas, MD
A fracture of the tibial
tubercle when associated
with a fracture of the tib-
ial plateau often disrupts
the extensor mechanism
and can be difficult to manage. Tradition-
ally, tibial tubercle fractures have been
repaired by lagging the tubercle fragment
to the posterior cortex of the tibia. How-
ever, the screws do not get adequate pur-
chase, particularly in comminuted or os-
teoporotic bone. Over several years we
successfully stabilized such tubercle frac-
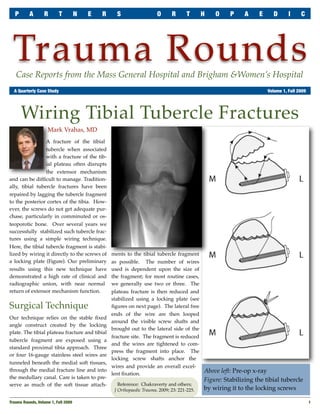
tures using a simple wiring technique.
Here, the tibial tubercle fragment is stabi-
lized by wiring it directly to the screws of ments to the tibial tubercle fragment
a locking plate (Figure). Our preliminary as possible. The number of wires
results using this new technique have used is dependent upon the size of
demonstrated a high rate of clinical and the fragment; for most routine cases,
radiographic union, with near normal we generally use two or three. The
return of extensor mechanism function. plateau fracture is then reduced and
stabilized using a locking plate (see
Surgical Technique figures on next page). The lateral free
ends of the wire are then looped
Our technique relies on the stable fixed
around the visible screw shafts and
angle construct created by the locking
brought out to the lateral side of the
plate. The tibial plateau fracture and tibial
fracture site. The fragment is reduced
tubercle fragment are exposed using a
and the wires are tightened to com-
standard proximal tibia approach. Three
press the fragment into place. The
or four 16-gauge stainless steel wires are
locking screw shafts anchor the
tunneled beneath the medial soft tissues,
wires and provide an overall excel-
through the medial fracture line and into Above left: Pre-op x-ray
lent fixation.
the medullary canal. Care is taken to pre- Figure: Stabilizing the tibial tubercle
serve as much of the soft tissue attach- Reference: Chakraverty and others;
J Orthopaedic Trauma, 2009; 23: 221-225. by wiring it to the locking screws
Trauma Rounds, Volume 1, Fall 2009
1
2. P A R T N E R S O R T H O P A E D I C T R A U M A R O U N D S
Post-operative Care
Patients are maintained at touch down
weight bearing in a range of motion brace
for six weeks to protect the plateau, but
are allowed full, active, and passive range
of motion from day one.
Key Learning Points
Use a proximal tibia locking plate for this
kind of operation. Whether the cerclage
wires used to tie down the tubercle are
placed before or after the locking plate is
not important. The critical factor is that
the wires pass around locking screws.
Right top: Wires are tunneled and
passed around screw shafts
Right below: Fragment is reduced
into place by tightening the wires
Far right: Post-operative x-ray
Trauma Faculty
Mark Vrahas, MD — 617-726-2943 Dear Co!eague:
Partners Chief of Orthopaedic Trauma
mvrahas@partners.org Thank you for taking the time to read the first edition of Partners Orthopaedic
Mitchel B Harris, MD — 617-732-5385 Trauma Rounds. We hope these Rounds provide you with useful information that
Chief, BWH Orthopedic Trauma you can apply to your practice.
mbharris@partners.org
R Malcolm Smith, MD, FRCS — 617-726-2794 We plan to publish quarterly both on paper and on our website:
Chief, MGH Orthopaedic Trauma http://achesandjoints.org/Trauma. Each issue wi! feature an article authored by
rmsmith1@partners.org
one of our Partners Orthopaedic Trauma faculty, whom you wi! be able to con-
David Lhowe, MD — 617-724-2800 tact directly with your questions and feedback.
MGH Orthopaedic Trauma
dlhowe@partners.org
The Partners Orthopaedic Trauma Service is a combined clinical and academic
David Ring, MD — 617-724-3953 entity which spans the campuses of the Massachusetts General Hospital and
MGH Hand & Upper Extremity Service
dring@partners.org Brigham & Women’s Hospital. This year, we celebrate our Tenth Anniversary.
George Dyer, MD — 617-732-6607 We could not have come this far without your support – our partners in the com-
BWH Hand & Upper Extremity Service munity.
gdyer@partners.org
In this new venture, we welcome your comments and su'estions for future topics.
Program Director
Suzanne Morrison, MPH Best regards,
(617) 525-8876
smmorrison@partners.org
Please send correspondence to:
Trauma Rounds Editor in Chief Editor, Publisher
Yawkey Center for Outpatient Care, Suite 3C
Mark Vrahas, MD Arun Shanbhag, PhD, MBA
55 Fruit Street, Boston, MA 02114
2
Trauma Rounds, Volume 1, Fall 2009