Downloaded 49 times










![Codeine and PM
• Purple Drank is an illegal recreational drink
popular amongst the hip-hop community of
the Southern United States. Its main
ingredient is prescription-strength cough
syrup containing codeine and
promethazine.[1]](https://image.slidesharecdn.com/web-onlyrx15lewed4301mollica2clark-150402163247-conversion-gate01/85/Web-only-rx15-le_wed_430_1_mollica_2clark-33-320.jpg)









![ETIZOLAM
• As of August 2014 Etizolam is not authorized for
medical use in the U.S. However, it currently
remains unscheduled and is legal for research
purposes. As its closest derivative is a Schedule IV
drug under Federal Scheduling Guidelines, it does
not fall under the Federal Analog Act, which only
applies to Schedule I and II drugs.
• The state of Arkansas has proposed listing
Etizolam as a Schedule I drug under their drug
scheduling guidelines] along with the state
of Mississippi .](https://image.slidesharecdn.com/web-onlyrx15lewed4301mollica2clark-150402163247-conversion-gate01/85/Web-only-rx15-le_wed_430_1_mollica_2clark-55-320.jpg)






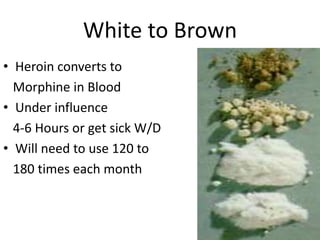
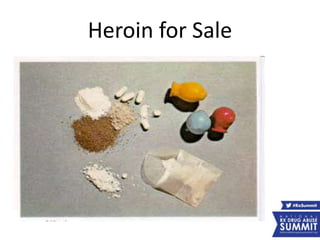
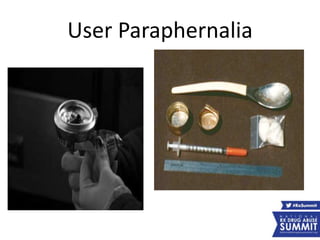
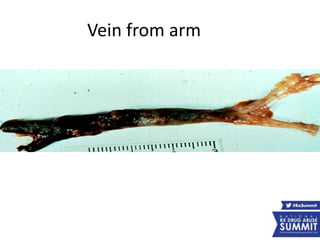
This document summarizes a presentation on trends in drugs of choice. It discusses the transition from prescription opiate abuse to heroin use. Presenters include experts from law enforcement and addiction medicine. The presentation covers learning objectives on identifying abused opiates and signs of heroin use. It also explains treatment methods for heroin addiction, describing it as a chronic brain disease requiring long-term, multi-faceted treatment approaches.