Downloaded 18 times






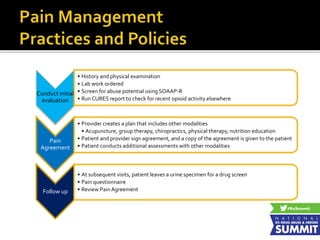

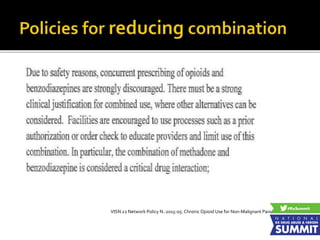
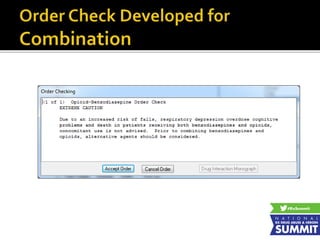


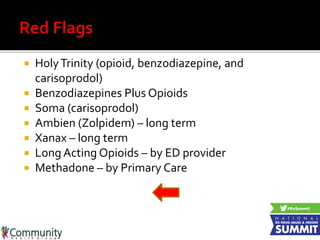
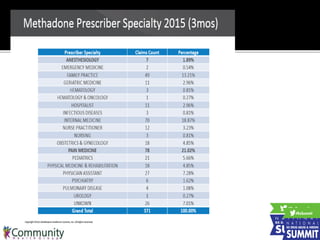





This document summarizes a presentation on health plan involvement in safe prescribing. It includes: 1) Presentations from medical experts on prescription drug abuse trends from medical examiner data and a tribal health system's safe prescribing program. 2) A discussion of health plan policies to reduce "red flag" medication combinations like opioids plus benzodiazepines through prior authorization, formulary changes, and provider restrictions. 3) Examples of one health plan's implementation of policies like restricting methadone prescriptions to pain specialists and removing carisoprodol from its formulary.






















































































