Downloaded 74 times



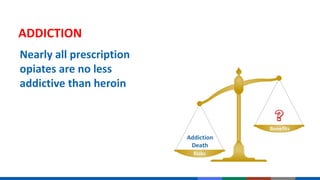
![Initiation of treatment with
opioids is a momentous decision
and should be undertaken only
with full understanding by both
the physician and the patient of
the substantial risks involved
MOMENTOUS DECISION
Frieden TR, Houry D. Reducing the Risks of Relief – The CDC Opioid-Prescribing Guideline. N Engl J Med. 2016 Mar 15. [Epub ahead of print].](https://image.slidesharecdn.com/q52zafmsbuodqqjxlpae-signature-537a65255b5399c187e949822e0c31366b84fba834565324fb8094b900831f29-poli-160414204454/85/Dr-Tom-Frieden-keynote-24-320.jpg)







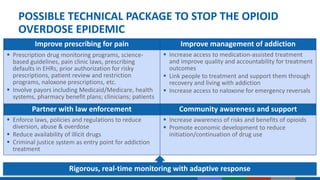
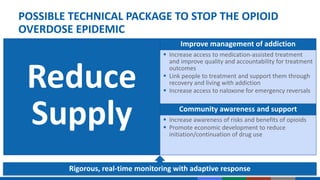
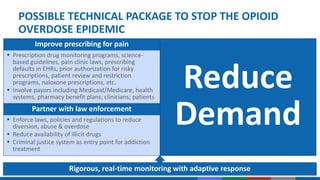
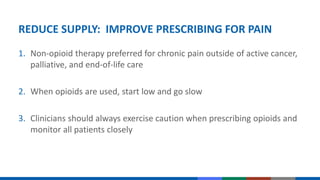
The document presents a comprehensive overview of the opioid epidemic, highlighting a significant rise in drug overdose deaths and the need for improved management and treatment strategies. It calls for a multifaceted approach involving better prescribing practices, increased access to medication-assisted treatment, community awareness, and enforcement of regulations to combat both prescription and illicit opioid abuse. The document emphasizes collaboration across health systems, law enforcement, and communities to effectively address the crisis and prevent further addiction and overdose incidents.