Downloaded 22 times









































































































































































































































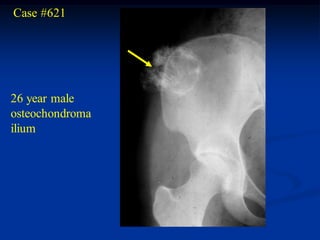

























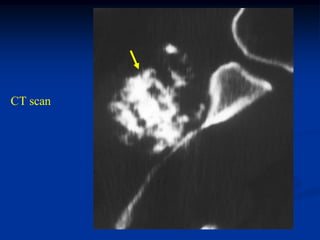






























































































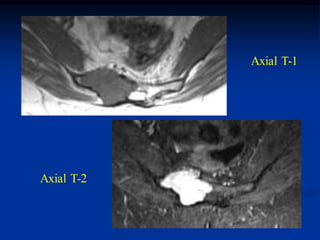


Osteochondroma is one of the most common benign bone tumors. It originates from the growth plate and continues growing during development, stopping at maturity. It is made up of a bony base with a pedunculated stalk containing fatty marrow and a cartilaginous cap. Solitary osteochondromas usually arise from large bones like the knee, femur, and humerus. Multiple hereditary osteochondromas present with multiple lesions and are inherited. Malignant conversion of a solitary osteochondroma can occur in adults but is extremely rare.
















































































