OSTEOCHONDROMA
• Osteochondroma isa bony exostosis projecting fro the external surface of bone
• It usually has hyaline lined cartilaginous cap.
• Incidence – 20 to 50% of all primary benign bone tumour
• Common in males, second decade of life
• Predisposing factors – Total body radiotheraphy, salter harris fracture and
surgery
• Location – Metaphysis of long bones > flat bones
• Long bones – Distal femur > Proximal humerus, proximal tibia, proximal femur
• Short bones – Ilium, scapula, ribs
7.
TYPES
• By number
1.One bone – Solitary osteochondroma
2. Two or three bones with no family history – Multiple osteochondromas
3. Multiple bones with family history – Hereditary multiple exostoses (Diaphyseal aclasis)
• By morphology
1. Pedunculated – Exhibits a base that has an elongated bony stalk merging continuously with
host bone. Common in bones around knee, hip and ankle
2. Sessile – plateau like stalk producing a broad base protuberance. Common in proximal humerus
and scapula.
9.
SYMPTOMS
• Mostly asymptomaticnunlessthey disturb adjacent blood vessels,
nerve or joint function.
• Hard painless mass near a joint
• Fracture through the stalk – severe pain and swelling
• Large spinal osteochondroma – cord compression, sciatica and
scoliosis
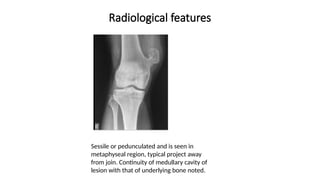
Radiological features
Sessile orpedunculated and is seen in
metaphyseal region, typical project away
from join. Continuity of medullary cavity of
lesion with that of underlying bone noted.
12.
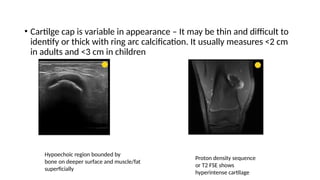
• Cartilge capis variable in appearance – It may be thin and difficult to
identify or thick with ring arc calcification. It usually measures <2 cm
in adults and <3 cm in children
Hypoechoic region bounded by
bone on deeper surface and muscle/fat
superficially
Proton density sequence
or T2 FSE shows
hyperintense cartilage
13.
Malignant osteochondroma
Malignancy issuspected when
• Growth after skeletal maturity
• Cortical destruction
• Increasing pain and mass
• Soft tissue mass
• Thick irregular calcified cap
• Cartilage cap > 2 cm in adults, > 3 cm in children.
14.
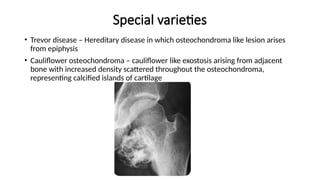
Special varieties
• Trevordisease – Hereditary disease in which osteochondroma like lesion arises
from epiphysis
• Cauliflower osteochondroma – cauliflower like exostosis arising from adjacent
bone with increased density scattered throughout the osteochondroma,
representing calcified islands of cartilage
15.
Hereditary Multiple exostosis
•Autosomal dominant disorder characterized by multiple
osteochondromas(Average 10)
• Common sites – Long bones of knee, ankle, shoulder and wrist. Flat
bones involvement is rare.
• Distribution is usually bilateral and symmetric
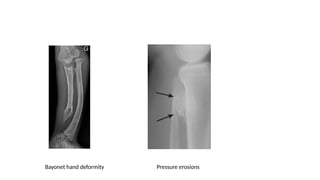
• Radiological features – Multiple osteochondromas, Bayonet hand
deformity, pressure erosions to adjacent bones
Treatment
• Asymptomatic –No treatment
• Symptomatic / Risk of malignancy – Surgical resection with care taken
to include periosteal surface
18.
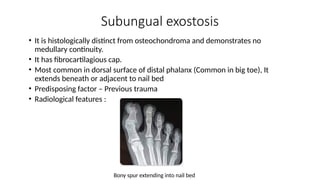
Subungual exostosis
• Itis histologically distinct from osteochondroma and demonstrates no
medullary continuity.
• It has fibrocartilagious cap.
• Most common in dorsal surface of distal phalanx (Common in big toe), It
extends beneath or adjacent to nail bed
• Predisposing factor – Previous trauma
• Radiological features :
Bony spur extending into nail bed
19.
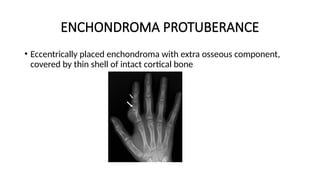
ENCHONDROMA
• It isan intramedullary neoplasm comprising lobules of benign hyaline
cartilage.
• Incidence – 10% of all benign bone tumours
• Common in age 10 – 30 years , equal in both males and females.
• Location – Tubular bones of hands and feet (Proximal phalanges >
metacarpals > middle phalanges)
• Other sites – Femur, tibia and humerus.
• Symptoms – Mostly asymptomatic but can present with pathological
fracture
• Can rarely lead to chondrosarcoma
20.
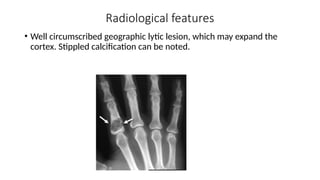
Radiological features
• Wellcircumscribed geographic lytic lesion, which may expand the
cortex. Stippled calcification can be noted.
21.
• Sharply definedmargins
• Size <5cm
• Narrow zone of transition
• Endosteal scalloping
• Thinned cortex
• Ring and arcs calcification
• No bone destruction, periosteal reaction or soft tissue mass
22.
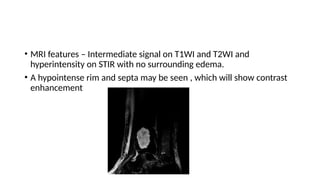
• MRI features– Intermediate signal on T1WI and T2WI and
hyperintensity on STIR with no surrounding edema.
• A hypointense rim and septa may be seen , which will show contrast
enhancement
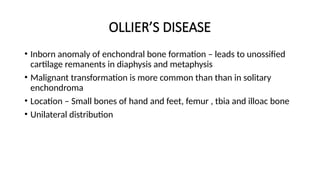
OLLIER’S DISEASE
• Inbornanomaly of enchondral bone formation – leads to unossified
cartilage remanents in diaphysis and metaphysis
• Malignant transformation is more common than than in solitary
enchondroma
• Location – Small bones of hand and feet, femur , tbia and illoac bone
• Unilateral distribution
26.
Maffucci syndrome
• Characterisedby multiple enchrondromas and soft tissue cavernous
hemangiomas
• Malignancy is more common here than in ollier’s disease
27.
Periosteal chondroma
• Slowgrowing benign cartilaginous tumour that develops within and
beneath the periosteum on the surface of cortical bone
• Common in young adults
• Common sites – Small bones of hand and feet
• Other sites – Femur, tibial, radius, ulna and fibula
28.
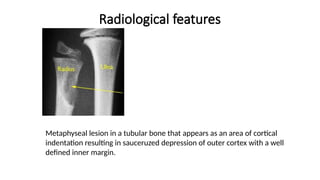
Radiological features
Metaphyseal lesionin a tubular bone that appears as an area of cortical
indentation resulting in sauceruzed depression of outer cortex with a well
defined inner margin.
29.
Synovial chondromatosis
• Alsoknown as Reichel syndrome
• Characterised by loose cartilaginous bodies which may or may not be
calcified
• Primary – Predominantly monoarticular disorder of unknown etiology
• Secondary – Osteoarthrosis, neuropathic arthropathy
30.
Chondromyxoid fibroma
• Rare,benign tumour of bone composed of chondroid, fibrous and
myxoid tissues
• Incidence - < 1% of all bone tumoours
• Age – 10 to 30 yrs and > 60 yrs.
• Commonn site- Bone around knee > humerus, ribs
• Symptoms – Evolving pain and occasional swelling
• Size – 1 to 10 cm (average 3 cm)
31.
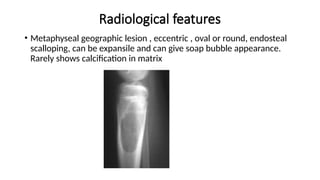
Radiological features
• Metaphysealgeographic lesion , eccentric , oval or round, endosteal
scalloping, can be expansile and can give soap bubble appearance.
Rarely shows calcification in matrix
32.
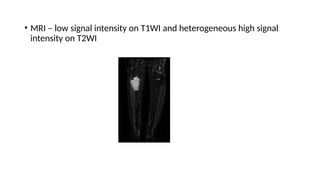
• MRI –low signal intensity on T1WI and heterogeneous high signal
intensity on T2WI
33.
Chondroblastoma
• Rare primarybenign tumour of cartilaginous origin.
• Usually seen before epiphyseal closure and primarily affects the long
tubular bones of lower extremities.
• Incidence - <1% of all bone tumours (550)
• 10 – 25 years of age, males
• Symptoms – pain aften reffered to adjacent joint, swelling and
tenderness, joint effusion, pathological fractures.
• Common sites – Proximal femur > distal femur > proximal tibia > proximal
humerus > tarsak bones
• Microscopy – Chicken wire calcification
• Can rarely have metastases to lung
34.
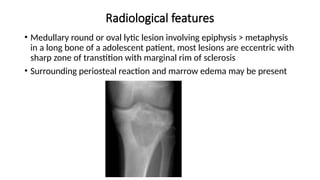
Radiological features
• Medullaryround or oval lytic lesion involving epiphysis > metaphysis
in a long bone of a adolescent patient, most lesions are eccentric with
sharp zone of transtition with marginal rim of sclerosis
• Surrounding periosteal reaction and marrow edema may be present
35.
MRI features
• T1– intermediate signal ,T2 – heterogeneous intermediate signal
• Hypointense sclerotic rim
• STIR – high signal
• Can have surrounding bone marrow and soft tissue edema
36.
Differential diagnosis
• Giantcell tumour
• Brodie’s abscess
• Eosinnophilic granuloma
• Treatment
• Curettage accompanied by packing with cancellous bone chips
OSTEOMA
• Benign bonetumour that arise from membranous bone
• Most are asymptomatic and their true incidence is unknown
• Common sites – Frontal and ethmoidal sinuses, outer and inner table
of skull
• If lesion interferes with drainage of sinuses – chronic sinusitis with
retro orbital pressure, headache, mucoceles and rarely leads to brain
abscess
• Most osteoma never reach a size of > 2 cm
• However these lesion rarely enlarge , filling a sinus completely(Giant
osteoma)
39.
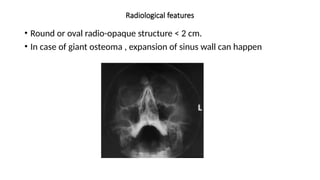
Radiological features
• Roundor oval radio-opaque structure < 2 cm.
• In case of giant osteoma , expansion of sinus wall can happen
40.
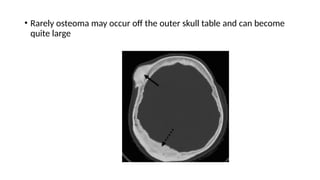
• Rarely osteomamay occur off the outer skull table and can become
quite large
41.
GARDENER’S SYNDROME
• Triadof multiple osteomas, colonic polyposis and soft tissue fibromas
• Common bones involved – frontal, mandible, maxilla, sphenoid,
ethmoid, zygoma and tubular bones of hand and feet.
42.
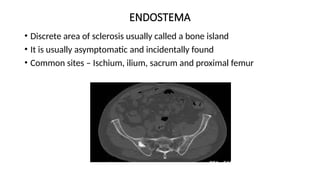
ENDOSTEMA
• Discrete areaof sclerosis usually called a bone island
• It is usually asymptomatic and incidentally found
• Common sites – Ischium, ilium, sacrum and proximal femur
43.
Osteoid osteoma
• Itis a small benign vascular osteoblastic ttumour is associated with
clinical picture of night pain relieved by NSAIDS
• Second or third decade, males
• Sites – Diaphysis of metaphysis of appendicular skeleton, more
common in femur or tibia
• Some of these lesions are intra articular causing synovitis and mono
arthropathy
44.
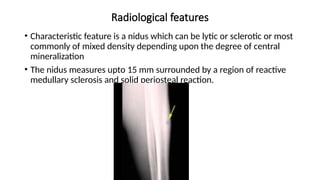
Radiological features
• Characteristicfeature is a nidus which can be lytic or sclerotic or most
commonly of mixed density depending upon the degree of central
mineralization
• The nidus measures upto 15 mm surrounded by a region of reactive
medullary sclerosis and solid periosteal reaction.
45.
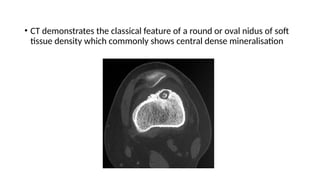
• CT demonstratesthe classical feature of a round or oval nidus of soft
tissue density which commonly shows central dense mineralisation
46.
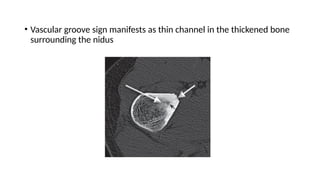
• Vascular groovesign manifests as thin channel in the thickened bone
surrounding the nidus
47.
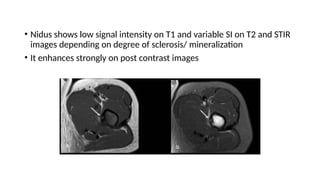
• Nidus showslow signal intensity on T1 and variable SI on T2 and STIR
images depending on degree of sclerosis/ mineralization
• It enhances strongly on post contrast images
48.
Treatment
• Most willhave spontaneous regression
• NSAIDS
• Surgery
• Radiotheraphy and thermocoagulation
49.
SPINAL OSTEOID OSTEOMA
•Most common - Lumbar spine
• Common site in spine – Neural arch
• Symptoms precedes radiological changes
• Vertebral body lesion can cause ivory vertebrae or focal sclerosis
• Adult
• osteoblasticmetastases
• prostate cancer
• breast cancer
• lymphoma (usually Hodgkin lymphoma)
• tuberculous spondylitis
• hemangioma
• chordoma
• Paget disease of bone
• vertebral body expansion (unlike hemangioma)
• coarsened trabeculae
53.
OSTEOBLASTOMA
• Rare benignneoplastic lesion
• Incidence <1 % (400) , 10-20 yrs, males
• It is termed as giant osteoid osteoma
• Symptoms – Pain (Neither nocturnal nor relieved by NSAIDS), scoliosis
provoked by pain, parasthesias and weakness
• Location – Spine > femur > foot and ankle > ribs > others
• In spine , neural arch is commonly involved. Upper thoracic and lower
lumbar is commonly involved.
• Nidus is usually > 2 cm and softer than of osteoid osteoma
54.
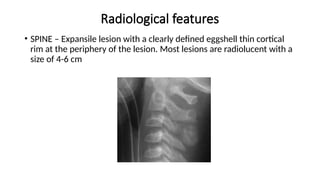
Radiological features
• SPINE– Expansile lesion with a clearly defined eggshell thin cortical
rim at the periphery of the lesion. Most lesions are radiolucent with a
size of 4-6 cm
55.
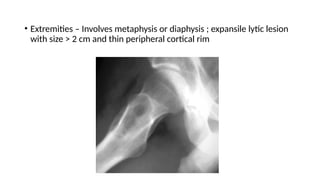
• Extremities –Involves metaphysis or diaphysis ; expansile lytic lesion
with size > 2 cm and thin peripheral cortical rim
56.
TREATMENT
• Small lesion– surgery and curettage
• Spinal lesions are often inoperable and requires radiation theraphy
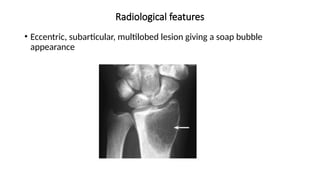
Giant cell tumour
•GCTs are locally aggressive neoplasm that orginates from non bone
forming supporting connective tissue of marrow.
• This highly vascular tumour is composed of spindle shaped stromal
cells interspread among multinucleated giant cell.
• Some of these tumours can be malignant
• It accounts for 15% of all benign bone tumours and 5-8% of all
primary malignant bone tumour
• 20-40 years, female
• Symptoms – aching pain with localized swelling and tenderness,
pathological fractre
59.
• Location- Distalfemur > proximal tibia > distal radius > proximal
humerus > others
• Involvement of distal radius causes a more series prognosis as most of
the lesions are malignant
• Sacrum is the most common spinal site
• These lesion usually begins in metaphyseal end of a long bone and
extends to the end of a long bone abutting its joint surface leaving the
lesion subarticular
TREATMENT
• Treatment ofchoice is surgical curettage combined with liquid
nitrogen freezing, bone packing or grafting
• Spinal lesions are often inoperable and needs radiotheraphy
• Prognosis is good for benign wheras for malignant tumour only 10% 5
year survival rate.
62.
Desmoplastic fibroma
• Rarelocally aggressive benign bone tumour which is considered as
counterpart of soft tissue desmoid tumour
• 0.3% of all benign bone tumours
• Common in young adults
• Common sites – mandible, metaphysis and diaphysis of long bone,
pelvis
63.
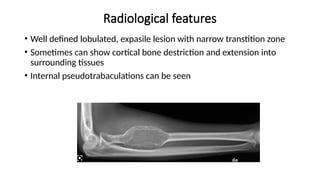
Radiological features
• Welldefined lobulated, expasile lesion with narrow transtition zone
• Sometimes can show cortical bone destriction and extension into
surrounding tissues
• Internal pseudotrabaculations can be seen
64.
Non ossifying fibroma
•They are benign osteoclastic neoplasm
• Second decade, males
• Most are asymptomatic and found incidently
• However large lesions >8 cm, can cause persistant pain and
pathological fractures
• Location – Distal tibia > proximal tibia, distal femur, fibula and
proximal humerus
• Most lesions are dimetaphyseal and eccentric in position
• Multiple non ossifying fibromas are found in neurofibromatosis
65.
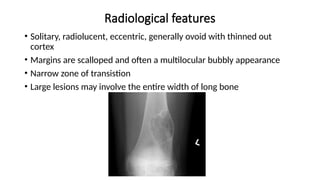
Radiological features
• Solitary,radiolucent, eccentric, generally ovoid with thinned out
cortex
• Margins are scalloped and often a multilocular bubbly appearance
• Narrow zone of transistion
• Large lesions may involve the entire width of long bone
66.
HEMANGIOMA
• It isa vascular solitary neoplasm that is slow growing and composed
of newly formed capillary, cavernous or venous blood vessel
• Represents 1% of all primary benign bone tumours
• Most common benign tumour of spine
• Age < 40 yrs, females
• Symptoms – Mostly asymptomatic, can cause localized pain and
surrounding muscle spasms, neurological compromise due to spinal
stenosis
• Location – Spine (lower thoracic and upper lumbar) and skull >
mandible, maxilla, petalla, metacarpals, ribs , scapula
67.
• Capillary hemangioma– Fine capillary loops tend to spread outward
in a sunburst fashion , when present , is usually encountered in flat
bones and metaphyseal ends of long bones
• Cavernous hemangioma – Large thin walled blood vessels and sinus
surrounded by a resorbed bony trabeculae. It is most common type
and frequently involves skull and spine
68.
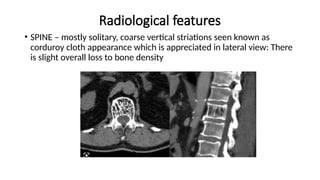
Radiological features
• SPINE– mostly solitary, coarse vertical striations seen known as
corduroy cloth appearance which is appreciated in lateral view: There
is slight overall loss to bone density
69.
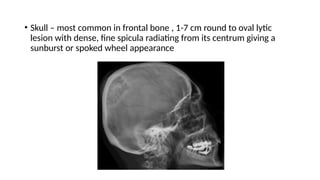
• Skull –most common in frontal bone , 1-7 cm round to oval lytic
lesion with dense, fine spicula radiating from its centrum giving a
sunburst or spoked wheel appearance
70.
TREATMENT
• Most lesionnned no treatment
• In lesions causing spinal stenosis, cord decompression should be done
• Radiation treatment can be given in inoperable vertebral
hemangioma
71.
INTRAOSSEOUS LIPOMA
• Primaryintraosseous lipoma is a rarest benign bone tumour (200).
• Soft tissue and subperiosteal lipomas are more common and can
secondarily involve the skeleton by extrinsic pressure on the cortex
• 4th
decade with no sex predilection
• Location – metaphysis of long bones particularly tibia and fibula,
calcenous and metatarsals
Simple bone cyst
•It is otherwise called as unicameral bone cyst or juvenile bone cyst is
not a true neoplasm of bone
• It is fluid filled cyst lined by a thin fibrous layer
• Age – 3 to 14 yrs, males
• Symptoms – Asymptomatic wntil they undergo pathological fracture
(2/3)
• Location – Proximal humerus and proximal femur > fibula, tibia,ribs,
pelvis , calcaneum, sacrum and clavicle
• Site – metaphysis immediately adjacent to epiphyseal cartilage plate
• Most lesion are central, with long axis parallel to long axis of bone
74.
Radiological features
• Cysticradiolucency that is broad at metaphyseal end and narrower at
epiphyseal end, long axis greater than diameter.
• A characteristic radiologic sign may be seen when a pathologic
fracture complicates this lesion – Fallen fragment sign and represent a
small, detached, floating bone fragment which will change position
within the lytic defect.
75.
TREATMENT
• Treatment ofchoice is surgical curettage with cauterization of cyst
• Packing of the hollow cavity with bone chips following surgery is
necessary
• Injection of steroids has significantly reduced the recurrence rates
76.
ANEURYSMAL BONE CYST
•ABC is a non neoplastic solitary lesion of bone containing a cystic
cavity filled with blood.
• The lesion is neither an aneurysm nor abone cyst but is made of
channels containing flowing blood
• Age – 5 to 20 years, female
• Symmptoms – pain with rapid increase in severity in a short period of
time, pathological fracture, spinal ABCs can cause neurological deficits
• Location – Long tubular bones (femur and tibia) and spine (Neural
arch) > Flat bones and short tubular bones
• Mostly affects metaphysis > diaphysis
77.
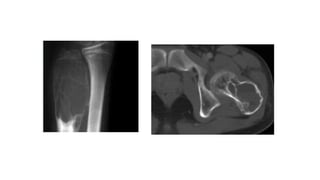
Radiological features
• Expansile,rapid growing , saccular lytic lesion, sharply demarcated by
thin subperiosteal shell
• Tends to be eccentric with multiple fine septa and sharply
demarcated, bulging , scalloping borders
• Many lesion may reach 8-10 cm and cause marked ballooning of a
thnned cortex - finger in the balloon sign.
• Periosteal new bone formation near the margins of lesion, creating a
buttressing effect
• On CT and MRI, several fluid levels can be seen within this lesion
owing to settling of degraded blood products
79.
FIBROUS DYSPLASIA
• Fibrousdysplasia is a developmental anamoly in which a defect in
osteoblastic differentiation and maturation results in replacement of
normal bone marrow with fibro-osseous tissue.
• Incidence – 7% of all benign bone tumours
• AGE < 30 yrs
• Symptoms – asymptomatic in case of no pathological fracture
• Common sites – Ribs > Proximal femur > Craniofacial bones
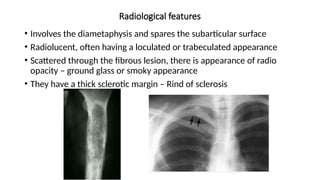
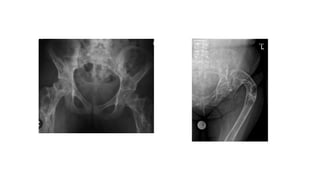
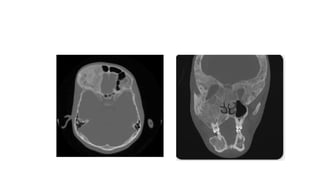
Radiological features
• Involvesthe diametaphysis and spares the subarticular surface
• Radiolucent, often having a loculated or trabeculated appearance
• Scattered through the fibrous lesion, there is appearance of radio
opacity – ground glass or smoky appearance
• They have a thick sclerotic margin – Rind of sclerosis
84.
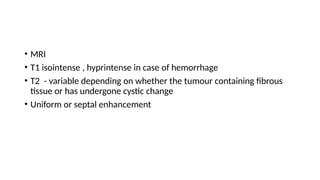
• MRI
• T1isointense , hyprintense in case of hemorrhage
• T2 - variable depending on whether the tumour containing fibrous
tissue or has undergone cystic change
• Uniform or septal enhancement
85.
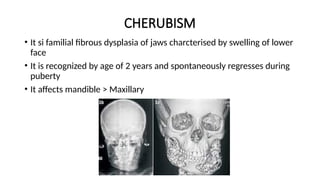
CHERUBISM
• It sifamilial fibrous dysplasia of jaws charcterised by swelling of lower
face
• It is recognized by age of 2 years and spontaneously regresses during
puberty
• It affects mandible > Maxillary