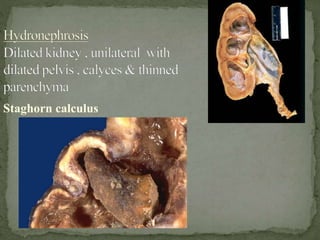
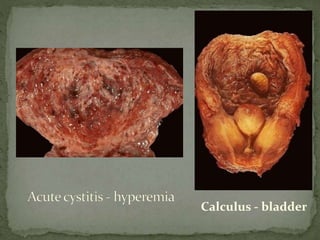
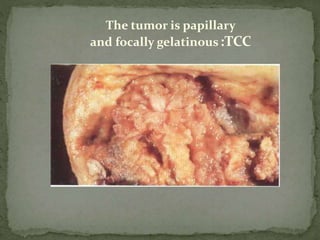
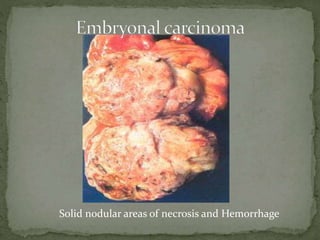
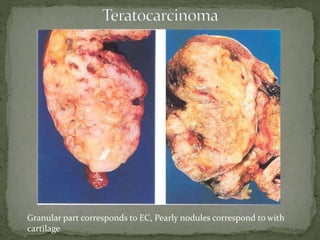
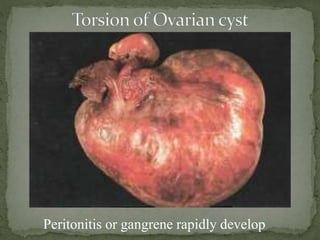
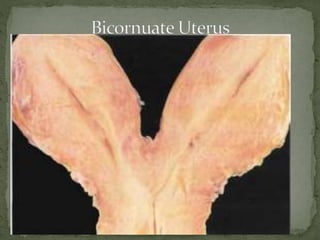
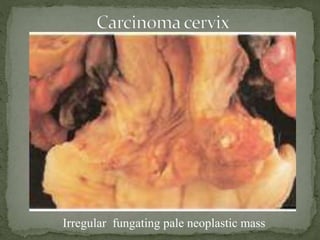
The document provides guidance on the proper dissection and examination techniques for various organs during an autopsy. It describes how to remove and examine the male and female reproductive systems, kidneys, bladder, prostate, testes, and other organs. Details are given on identifying congenital anomalies, diseases, infections and tumors that may be seen. Common findings for conditions like tuberculosis, infections, cancers, cysts and other pathologies are outlined. The document emphasizes thorough examination and documentation of pathological findings in organs.