Download to read offline






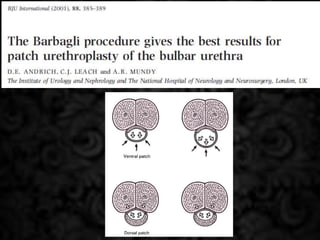
























1) The document discusses the reliability, simplicity, and outcomes of dorsal versus ventral grafting techniques for urethral stricture repair. 2) It notes that the dorsal approach may offer a wider graft placement and better conditions for graft survival. However, no single technique is best for all cases. 3) Outcomes data showed the dorsal grafting technique had a higher success rate, but more experience is still needed to conclude if dorsal or ventral positioning is clearly superior. Patient factors like stricture characteristics and comorbidities are also important to consider.























































































