This document provides an overview of basic ventilator mechanics including:
1) Definitions of mechanical ventilation, the types of mechanical ventilation including invasive positive and negative pressure ventilation, and the indications for mechanical ventilation.
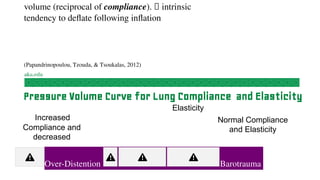
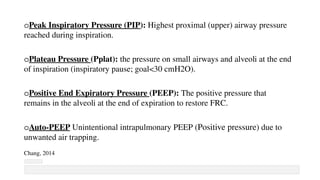
2) Basic ventilator terminology including lung compliance, elasticity, tidal volume, minute ventilation, inspiratory-expiratory ratio, and more.
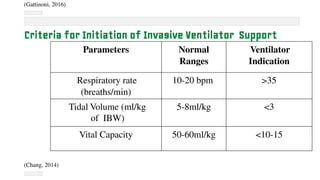
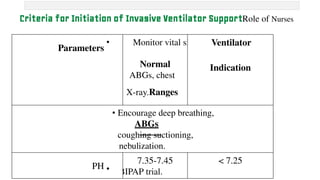
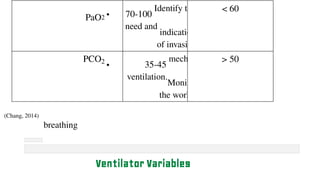
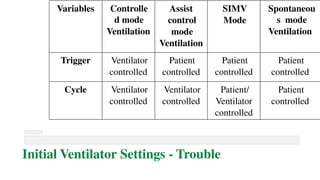
3) The criteria for initiation of invasive mechanical ventilation, types of breaths and modes of ventilation including controlled, assist-control, SIMV, and spontaneous/pressure support modes.
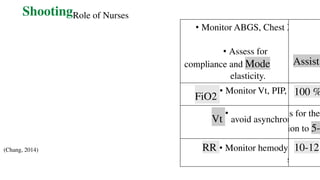
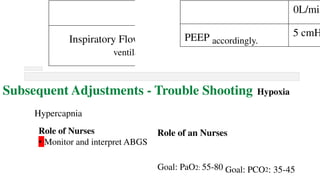
4) Initial ventilator settings and adjustments including factors like FiO2, tidal volume, respiratory rate, PEEP, and how to troubleshoot issues

![Terms and Definitions
o Tidal Volume (Vt): Amount of air passes in and out of lungs with each cycle.
(volume delivered with each preset breath)
o Minute Ventilation (VE): Volume of gas exchanged per minute [RR x TV]
o Inspiratory:Expiratory (I:E) Ratio: the ratio of inspiratory to expiratory
time determined by the speed of gas flow (1:2)
o Vital Capacity (VC): Maximum air expelled from lungs after a maximum
inhalation](https://image.slidesharecdn.com/ventilatormechanicsandinvasivemechanicalventilation-240225163521-fbdd775f/85/Ventilator-mechanics-and-invasive-mechanical-ventilation-pdf-9-320.jpg)































![Mechanical_ventilation[_fellow[1][1][1][1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/mechanicalventilationfellow1111-240923152440-d96712e3-thumbnail.jpg?width=640&height=640&fit=bounds)

























